
3757
Views & Citations2757
Likes & Shares
Poverty-Global Scenario [3-7]
Poverty is defined as a condition in which an individual or household lacks the financial resources to afford a basic minimum standard of living. The World Bank (WB) defines poverty as deprivation in well-being comprising many dimensions.
The WB sets three poverty lines. These are given below:
- International Poverty Line- $1.90 per day
- The second is for Lower Middle-Income Countries at $3.20 per day
- The third is Upper Middle-Income Countries at $5.50 per day
Poverty-National Scenario [3-7]
The post intervention study will focus on BPL families. Hence, in the back ground & rationale, poverty also needs to be discussed as it is also a state of health as per epidemiology. Like anemia, the nation has also travelled to reduce poverty. The first measurement of poverty was in 1867-68 prices. It was followed up by establishment of National Planning Committee in 1938. Subsequently, the Bombay plan followed & in 1962, it was quantified for the first time in independent India. After that, it journeyed through 1977, 1989, 2005, 2009 & 2012. In 2020, NITI Aayog proposed MDPI model. The recent progress in reducing poverty in India from 2013-14 to 2022-2023 is highly encouraging. During this 9period, in our nation, according to NITI Aayog, about 25 crores or 250 million of individuals have exited from Multi-Dimensional Poverty (MPI).
Poverty in the Intervention Area [3-7]
It is significant to note that as per NITI Aayog, 36.65% of the population in the state of MP are poor. The state of MP has the fourth largest poor population in the country. As per the census, Alirajpur district has the most illiterates & has 71.3% population under the poverty bracket. The district of Jhabua has 68.86% of population who are poor. To add to that, Barwani district has the maximum number of malnourished children. As per the projected population, about 2.5 crore people are poor in the state of MP. This situation makes the rationale of the intervention further strong.
AMB [8]
The Anemia Mukt Bharat (AMB) program was launched with a target to bring the prevalence rate to1%. The 6*6*6 strategy of the currently operational AMB has 6 beneficiaries & out of these six, two categories match with AMB. The intervention’s categories that match with the AMB are the children in the age group of 6-59 months, lactating mothers & pregnant women. The below-mentioned Figure 1 gives the glance of AMB’.

Food fortification is a strategy under AMB & the current post intervention study is regarding the fortification salt known as DFS. The salt has Encapsulated Ferrous Fumarate that target to reduce the prevalence of anemia in the nation. That’s why it is rational to put the framework in this proposal related to the post intervention study with a 6month duration.
To deal with these issues of anemia, the Government of India used the food fortification & supplementation strategy to deal with the issue. In this context, Encapsulated Ferrous Fumarate (EFF) Double Fortified Salt (DFS) were used as supplements & fortified food in the states of Gujarat & West Bengal successfully. Seeing the success, Nutrition International in partnership with the Government of Madhya Pradesh started the pilot project using these two ingredients in 5 selected districts of Madhya Pradesh.
Morbidity & Mortality Issues Related to Anemia [1-8]
It is also observed that the anemia is more prevalent in rural areas. Anemia is also an important cause of maternal mortality in India. In India, out of about 25million births, approximately 1.6 million are born with birth defects. The prevalence of Neural Tube Defects (NTDs) is higher in India (4.7per1000livebirths) compared to the global prevalence (2.5per1000livebirths). Currently, every year about 100,000 babies are born with some form of NTDs.
A Prelude Related to the Intervention Study [1-8]
Since the tenth five year plan the Government of India has laid focus on staple food fortification for addressing micronutrient deficiencies. The Ministry of Women and Child Development (2006 & 2009) and Ministry of Consumer Affairs, Food and Public Distribution (2008 & 2014) have also directed the states for fortifying the food being used in the existing social safety net programs. While salt iodization is mandatory, staple fortification continues to remain as pilots except Gujarat and West Bengal. To encourage the use of Double Fortified Salt (DFS) in other states the Ministry of Health and Family Welfare (MoHFW), Government of India has advised the Governments of state and Union Territories to include Double Fortified Salt (DFS) in various feeding programs.
Many states have not yet included DFS in the social safety net, however, the Government of Madhya Pradesh expressed interest in introducing DFS in on pilot basis through Public Distribution System (PDS) in 89 tribal blocks of 20districts and Nutrition International (NI) worked in a sub-set of 38 blocks of 5 districts.
Initially in the demonstration phase during a period of two years from 2018-19 to 2019-20, the DFS intervention aims at promoting consumption and increase coverage of EFF double fortified salt among the women of reproductive age (WRA) and adolescent girls through PDS and to examine the association between DFS and prevalence of anemia. To facilitate the implementation of DFS, NI provided technical assistance to the Government of MP. The state government sold one kilogram of DFS at INR1 or 2 per family per month through PDS and has a plan to replace the currently sold iodized salt to the DFS based on the success of the pilot.
NI hired an implementing NGO partner which provided trainings to state, division and district level health and civil supplies officials & built their capacities on forecasting, supply chain management, monitoring, reporting of the intervention and quality control on DFS. NI developed prototypes of IEC/BCC materials and carry out communication activities & built awareness of the community regarding benefits of DFS for its increased usage.
NI also did the evaluation of the DFS project. As part of this evaluation, NI conducted a program evaluation to measure anemia levels among non-pregnant women of reproductive age along with associated factors and knowledge and practices with respect to use of any iron and folic acid supplementation, iron rich food especially the double fortified salt. For this purpose, NI seeked the services of a competent research agency that has experience in drawing and analyzing blood samples and conduct community-based health and nutrition surveys.
The baseline survey of the above-mentioned pilot was done in October to December 2018 & the end line survey was done in the period Dec 2020 to Feb 2021.
The current post intervention is done after a period of 3 years after the end line. The duration of the post intervention is 6 months i.e. starting from March 2024 till August 2024. The proposal gives the current status of the 5 districts through the latest NFHS 5 survey as a secondary data. The proposal also focuses on the intervention through a focus on behavior change communication both from the user (demand) side & supply side of DFS & EFF.
OBJECTIVE OF THE STUDY
This post intervention study will measure the contribution of consuming DFS by nonpregnant women of reproductive age in households living below poverty lines towards reducing anemia level among population group in five districts of Madhya Pradesh state in India.
The overall objective of the post intervention study is to assess the effectiveness of DFS in improving anemia among the population group in the selected districts of Madhya Pradesh. To achieve the overall objective of the post intervention study, the agency will conduct the post intervention study in all the five selected districts where the piloting was done for a period of 3 years.
Specific Objectives & Research Questions (RQ) of the post intervention study
- Assess the contribution of regular consumption of DFS towards change in prevalence of anemia and iron deficiency anemia among non-pregnant women or women in the reproductive age WRA (15-49years).
The RQ under this objective is-What are the factors that lead to regular consumption?
- Assess the coverage and type of salt used among non-pregnant WRA (15-49years).
The RQs under this objective are- where is the level of coverage more?
What type of salt is popular among consumers?
- Assess the acceptability of EFF double fortified salt among consumers.
The RQ under this objective is- How do the acceptability of DFS increase?
- Assess knowledge-levels of consumers on anemia and how the same could be reduced by regular consumption of nutritious food including EFF
The RQ under this objective is- What is the current level of the status of knowledge among consumers?
How do they see dietary sources & DFS together to deal with anemia?
- Assess the availability and regular and adequate receipt of double fortified salt by consumers through public distribution system (PDS) and to provide suggestions to bridge the DFS supply gaps in
The RQs under this objective are- How the supply chain is maintained?
What are the steps taken to address the supply gaps?
- To understand the different sources of iron from daily or weekly iron and folic acid supplementation, iron-rich food intake, iron fortified from wheat, rice, milk, oil, ghee etc., will also be enquired to understand the level of iron load among the study population through a food frequency-based research tool.
The RQ under this objective is- How & when the community values the local food frequency calendar as a tool to deal with anemia?
- Understand the willingness of fair price shop owners and block and district health, nutrition (Integrated Child Development Services-ICDS) and PDS officials to counsel the women of reproductive age and other relevant stakeholders for using double fortified salt and making them aware of its
The RQ for this objective is- what are the motivating factors for the stake holders to counsel consumers & how will they do it?
Current Situation of Anemia in the 5 Selected Districts of MP
The following Table 1 gives the details of the districts of MP regarding the status of anemia as per NFHS 5. As the post intervention study is done after the end of end line evaluation in February 2021, it is prudent to use the updated data of NFHS 5 of 2019-2021 [1].
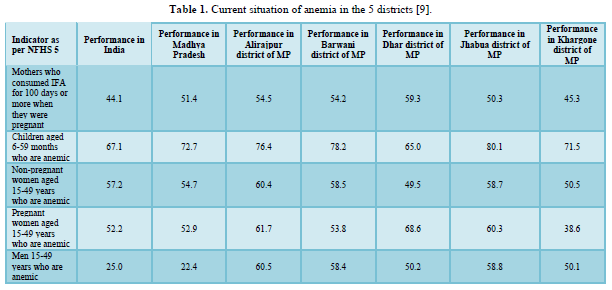
As we can see in the Table 2, Khargone is the district that has the poorest performance among consumption of IFA tablets in pregnant women. Similarly, Jhabua has the greatest number of anemic children in the age group of 6-59 months. Alirajpur district has the greatest number of non-pregnant women who are anemic. Dhar district has the maximum number of anemic pregnant women. Among men, again Alirajpur district has maximum number of men who are anemic.
Using the analogy of poor performance in these indicators, the sampling size of the respondents in these districts will be in line with the performance.
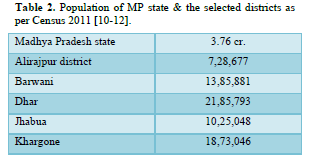
Another suggestional analogy to be used will be the population of the districts. The most populated district is Dhar. Hence, the sample size of Dhar district will be the maximum among the five districts. Alirajpur will have the smallest sample size. The second most sample size will be of Khargone district. The third most sample size will be from Barwani & the fourth in the row will be from Jhabua district.
Another analogy to categorize the districts will be the list of aspirational districts. Currently, in MP state, Barwani is the only aspirational district among the 5 districts. Hence, special focus has to be there during the intervention study as it is a backward district among the 5 selected districts. The current study deals with BPL families & this indicator is directly proportional with the aspirational district program of GOI.
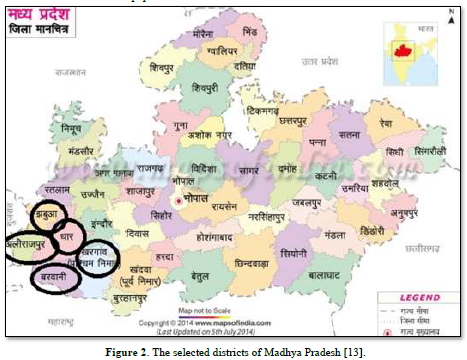
About the Project Locale [11,12]
The following Figure 2 of MP districts shows all the 5 districts of the state of Madhya Pradesh. The five selected districts of Madhya Pradesh as in the map of the state of MP. All the five districts are in the west MP. The districts lie in Indore division & Malwa region of MP & are adjacent to each other.
Alirajpur district comprises six tehsils and these are the six development blocks of the district. The names are Alirajpur, Jobat, Sondwa, Udaigarh, Chandra Sekhra Ajad Nagar and Kathiwada. Additionally, there are two Madhya Pradesh Vidhan Sabha constituencies in this district & these are Alirajpur and Jobat.
Barwani district is divided into two sub-divisions, Barwani and Sendhwa, which are further divided in to nine tahsils, Barwani, Sendhwa, Pansemal, Warla (Varla) Niwali, Thikri, Pati, Anjad and Rajpur, and seven developmental blocks, Barwani, Pati, Sendhawa, Pansemal, Niwali, Thikari and Rajpur.
Similarly, Dhar district has 13 blocks & Khargone has 9 blocks.
Jhabua district was divided into two parts in May 2008, namely Alirajpur and Jhabua. Alirajpur, Jobat, Udaigarh, Bhabra, Sondawa and Kathiwada are the 6 blocks of new district, Alirajpur. Jhabua district now consists of Jhabua, Meghnagar, Ranapur, Rama, Thandla & Petlawad blocks.
RESEARCH METHODOLOGY [14]
The sampling will be in stages. The first stage of sampling will be a non-probability sampling. The sampling technique to select the 5 districts is ‘Purposive’ as the piloting was done in these districts.
The second stage will be choosing the number of blocks in these districts. The following section gives the related details.
There are 13 blocks each in Dhar & Jhabua districts. There are 9 blocks in Khargone. There are 7 blocks in Barwani & 6 in Alirajpur.
Hence, 2 blocks each from Dhar & Jhabua will be selected randomly as these districts have the maximum number of blocks. One block each from the other three districts will be selected. So, in all, 7 blocks will be chosen randomly from the list of the blocks of the district.
On the basis of number of Below Poverty Line (BPL) families that are using the two ingredients through DFS, the household will be chosen using this information obtained from the PDS shops of the villages of the blocks. 5 such villages from each block will be listed & the 15-49-year group of men & women, pregnant women & mothers of 6-59 months old children will be listed & these categories become respondents.
So, the criteria to choose the villages will be based on the number of households that are consuming DFS & EFF. The villages showing the maximum numbers will be selected using the criteria of the selection of 5 villages that have the maximum users.
Sample size levels
- Community or Village level.
- Block level.
- District level.
Sample designs
A multi stage sampling design is applied in the current post intervention study.
PSU
The intervention study will have the selected villages as the Primary Sampling Units. There will be 35 villages in all that will be selected for the short study. 5 villages each from the 7 selected blocks make the N of the study to 35 villages. The total number of PSUs in the current intervention study is 35.
The respondents will be chosen in such a way that they represent the four directions of the block. Similarly, to have heterogeneity & better representation, all modalities like literacy, socio economic status & asset holding will be addressed.
RESPONDENTS
There are four categories of respondents from the demand side & these are mentioned below:
- Mothers who are in the age group of 15-49 years & are currently pregnant.
- Mothers who are in the age group of 15-49 years & are currently not pregnant.
- Mothers who have a child in the age group of 6-59 months.
- Men in the age group of 15-49 years.
There will be 5 mothers in each category & hence a total of 35*15= 525 mothers will be respondents.
Similarly, the total number of men respondents will be 35*5= 175.
Similarly, there will be three categories of respondents from the supply side. These are mentioned below:
- One PDS shop owner from each village.
- One block level official from the civil supply department.
- One district level official from the civil supply department.
N & n of the Pilot Study
- The total N for the study for the respondents is 650.
- Here the first n is 525 mothers.
- The second n is 175 men.
- The fourth n is 35 PDS shop owners.
- The fifth n is 7 block officials.
- The sixth n is 5 district officials.
Inclusion Criteria of the Respondents
- Those mothers who are purchasing the DFS from PDS shops & are consuming currently.
- Those mothers who are consuming EFF currently.
- Those men who consume DFS on a regular basis.
- Mothers who give their 6-59 months old children DFS on a regular basis.
- Those PDS shop owners who encourage & sell DFS currently.
- Those block & district officials who monitor the progress of the pilot currently.
- Few mothers & men from the selected villages to understand the barriers to behavior regarding adoption of DFS.
Exclusion criteria
- Mothers or women in 15-49year age group having conditions like haemoglobinopathies like sickle cell anemia or thalassemia.
- Men in 15-49year age group having conditions like haemoglobinopathies like sickle cell anemia or thalassemia.
- Mothers who are more than 49 years of age.
- Women who are less than 15 years of age.
- Men who are more than 49 years of age.
- Men who are less than 15 years of age.
Sampling weightage
Basically, sampling rule is 68-95-99. This means in 99, if out of 100 respondents, 99 respondents are selected, it is like census enumeration or100% enumeration. There is only one error in 100 respondents.
The second is 95 which mean in 100 respondents, there will be an error of 5. This means every 20th respondent, there is an error. There are 5 errors in 100 respondents.
The third is 68 which mean in 100 respondents, there will be error of 32. This means every 3rd respondent, there is an error. There are 32 errors in 100 respondents.
Since this is a short study with few sample sizes, the Confidence Interval in the post intervention study will be 68%.
Survey Design
The survey design used by NI to do the end line evaluation was ‘Experimental’ as they used an intervention & control group to assess the effectiveness of DFS in prevalence of anemia.
Analytical statistics like t test & chi square must have been used to ascertain the relationship among variables. If the research team had used hypothesis, the application could have been like the following.
Hypothesis
Here there are two variables in the proposed intervention study. The dependent variable is the mean hemoglobin concentration & the independent variable is the consumption of DFS. There can be three hypotheses that can be tested. These three are given below.
Null Hypothesis (H0)- There is no relation between the variables.
H1- There is a direct relationship among the variables
H2- There is an indirect relationship among the variables.
As reported in the end line of the study, the H1 was accepted & the null hypothesis was rejected.
The current post intervention study focuses on the behavior change aspects of DFS. Hence, the study design will be ‘Survey’ where one to one interaction with mothers & men will be through In-Depth- Interview (IDI) schedule will be done among the current users of DFS.
HYPOTHESES IN THE CURRENT POST INTERVENTION STUDY
As it is a study that focuses on behavior change regarding use of DFS on a regular basis, the hypotheses will be as per the following.
H0- Null Hypothesis-There is no resistance in the community regarding the regular use of DFS.
H1- Community prefer the DFS to the conventional iodized salt that they use
H2- Iodized salt is more preferable to the community members.
Understanding Barriers in the Process
Similarly, to understand the barriers of uptake & use of DFS on a regular basis, Focus Group Discussions (FGD) will be held among separate groups of men & women to elicit the barriers.
Next, interviews will be done with stakeholders or officials at village, block & district level using a short ‘Interview Guide’ to elicit the modalities on the supply side.
The next design that we can use in the post intervention study is ‘Case Study’. Here, one case study per block where the most active household using the DFS currently will be the respondent. Here the existing list of households will be the base for choosing the respondent.
Data
The post intervention study will use both types of data or mixed data approach. The quantitative data will be through the IDI. The qualitative data will be through the FGD & Case Studies.
Errors
As per the study, the mean prevalence of anemia is 12.0 grams/deciliter or 12 grams percentage. Estimation of anemia status by the respondents on their own will help us to know whether their hemoglobin is above the mean level. The Standard Error (SE) will be those above & below the prescribed level.
As explained above, the Sampling Error (SE) is 32 in 100 respondents or one error in every 3rd respondent.
Confidence Interval
The confidence interval of the post intervention study is 68%, below which CI is not permissible.
Limits
As per the age of adult respondents, the lower limit of respondents is 15 & the upper limit of respondents is 49 for men & women.
As per the age of mothers of children in 0-59 months also, the upper limit & lower limit remain the same as mothers are the respondents.
As per the mean levels of hemoglobin, which is here 12 grams per deciliter, the upper limit can be 16 grams per deciliter & the lower limit will be 8 grams per deciliter.
RESEARCH TOOLS
There are FOUR research tools to be used in the post intervention study. These are given below:
- In Depth Interview Schedule.
- Interview Guide.
- FGD protocol.
- Case Study outline on which case studies will be written.
It is expected that the IDI tool will consume the maximum time followed by the case study outline. The Interview Guide tool will consume the least amount of time. In between these tools, the FGD protocol use time will be there.
After the pilot, appropriate corrections will be made in the tools towards the finalization of tools.
Issues to be Addressed in Research Tools Development
The first section of all the research tools will be to assess the background of the respondents where their socio-economic status, literacy status, house hold profile, assets status will be dealt upon.
The first section of the research tool for the mothers will focus to assess the contribution of regular consumption of DFS towards change in prevalence of anemia and iron deficiency anemia among non-pregnant women or women in the reproductive age WRA (15-49 years).
The second section of the research tool of the mothers will focus to assess the coverage and type of salt used among non-pregnant WRA (15-49 years).
The research tool for the stake holders will focus to assess the acceptability of EFF double fortified salt among consumers.
The research tool for the mothers will also deal to assess knowledge-levels of consumers on anemia and how the same could be reduced by regular consumption of nutritious food including EFFDFS.
Another section of the research tool for stake holders or the supply side will be to assess the availability and regular and adequate receipt of double fortified salt by consumers through public distribution system (PDS) and to provide suggestions to bridge the DFS supply gaps in PDS.
Since it is a study based on behavioral aspects, the research tool for mothers will address to understand the different sources of iron from daily or weekly iron and folic acid supplementation, iron-rich food intake, iron fortified from wheat, rice, milk, oil, ghee etc., will also be enquired to understand the level of iron load among the study population through a food frequency-based research tool.
The research tool for the stakeholders representing the supply side will also be used to understand the willingness of fair price shop owners and block and district health, nutrition (Integrated Child Development Services-ICDS) and PDS officials to counsel the women of reproductive age and other relevant stakeholders for using double fortified salt and making them aware of its benefits.
RESEARCH TOOL & RESEARCH QUESTIONS
There are seven objectives & each objective has one or more than one objective. The answers to these research questions help us to achieve the objectives. The research tool’s sections will revolve around these RQs.
RESEARCH TOOL & REPORT WRITING
Each section of the research tool will be made a table in the final report. The tables will be both quantitative & qualitative data based.
The common theme in the FGD protocol & the findings will be clubbed while making the tables & against each of the finding, the number of respondents in that issue will be mentioned against the N & n.
Logical Frame Work
The INPUT here is the willing to purchase the DFS from PDS shop owners.
The OUTPUT here is the regular consumption at the household level.
The OUTCOME here is that the household that use DFS on a regular basis talks about its benefits & encourages another household to use DFS.
The IMPACT here is that regular users of DFS have achieved the mean level of 12 .0 grams of hemoglobin per deciliter of blood.
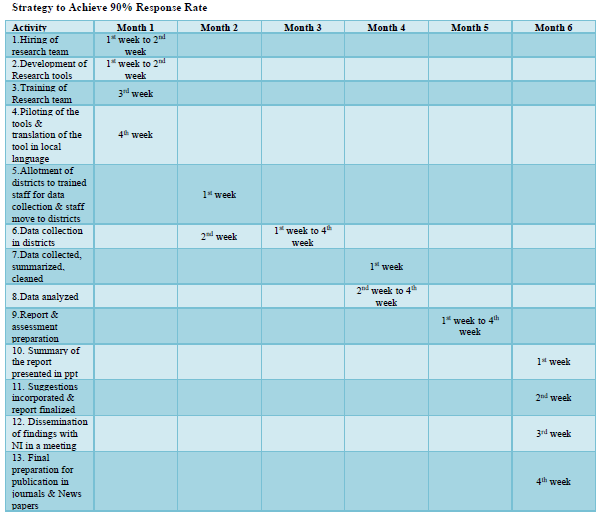
Strategy to Achieve 90% Response Rate
There will be at least 10 backup respondents in each PSU list so that if a selected respondent is unwilling, absent during data collection, the total of willing respondents remains the same.
Activity Plan of the Intervention
The total consultancy period is for 24 weeks or 6 months. The detailed activity plan is given per month & each week of the month in the following Table.
RESEARCH TEAM OF THE INTERVENTION
The post intervention study will consist of a research team that will be involved for a period of 6 months from month 1 to month 6. The following are the staff details:
- Trained staff on how to do the intervention- 20 staffs- 5 for each district.
- A nutrition epidemiologist with minimum 5 years of experience or a Masters in Nutrition with 10 years’ experience.
- One Monitoring & Evaluation expert with a Master’s degree with 5 years of experience & should have published articles.
- Statistician or Software developer with more than 5 years of experience.
Role of the Team Members
- The staffs will be responsible for data collection & reporting of the data.
- The nutrition epidemiologist will assess the methods, its application as per the prescribed guidelines.
- The M & E expert will focus on the change in performances that are ongoing on a regular basis, periodical basis & at the end of the intervention period. Collect, summarize & clean data.
- The statistician will use the descriptive & inferential statistics on the analyzed data. Also make the results statistically valid & reliable.
- The nutrition epidemiologist will oversee all the activities & lead the team as well.
Ethical Considerations [15]
At the state of MP, prior to survey, the permission for the ethical measures from the state level ethical committee will be sought. The intervention will adhere to the standard ethical protocol as set by the state level committee. The following measures will be adhered during the intervention.
Informed Consent & Assent Procedures
Consent or assent will be taken before conducting the interview of selected respondents. These respondents will be from families that are using DFS & EFF, families that are not using DFS & EFF so that we know the barriers for the intervention. It will consist of both men & women. Through the respondents who are mothers, the intervention will elicit the status of the children as well. Pregnant, non-pregnant & recently delivered women from these families will be the respondents.
The participant information sheet and consent/assent form will describe the purpose of the post intervention study, the survey procedures including interview, FGD. The potential risks and benefits of participation, the right to refuse participation or answer any question, measures to ensure confidentiality, will be included in the contact details for the research team. The forms will include consent/assent for the collection of survey interview & FGD data.
The consent/assent forms will be translated into state language of MP. A copy of the consent or assent form will be given to the mother/caregiver to read or will be read out if the participant was illiterate. Only after all questions were answered, the mother/caregiver will sign the consent/assent form. For illiterate participants, a thumb impression (right hand) will be taken in the presence of a witness.
RISKS AND BENEFITS
There are no foreseen significant risks from participating in the survey or from the collection of data. Research team training will focus on providing assurance to participants about their confidentiality and alleviating possible discomfort when answering potentially sensitive questions like past illness, socio-economic status, house hold sanitation facilities. Interviewers will be trained to elicit information in a non-judgmental way. Efforts will be also made to minimize discomfort during the data collection.
All survey data will be transmitted in formats that will not identify the study participant or household. No names, addresses or GIS information will be recorded or stored in the survey database.
Compensation/Incentives
No compensation will be provided for participating in the survey. Results if significant for each participant will be sent to them individually to their home address by India Post.
Mechanism for Quality Assurance-Internal Monitoring and Supervision [6]
The performance of the interviewers will be supervised at different levels. In each PSU, one supervisor and a data quality control observer will be deployed to supervise the team. The supervisor will be responsible for overall planning & coordination of the field work. They will also build rapport with the community, supervision of field work & report on PSU completion. They will also visit all sampled households & respondents. They will also compare the list of household members from the household listing to the original sample listing to ensure quality.
At the first level, at least 10% of the survey forms will be monitored to see that whether these required re-interviews or not.
A research team to assure quality will visit all the listed households & if they find error in the listing to more than 10%, the listing will be redone. The team will also observe two interviews in each PSU. The team will also conduct at least one interview to ensure quality.
The investigators will also receive a tab to collect & feed data. They will fill the data on the offline mode & upload the data on the online after verification at the end of the day.
A quality assurance team from NI will also visit the field during data collection to ensure quality.
The agency will also develop a field check table every week & share the feedback with the field team.
Deliverables as Per the Scope of Work
In a period of 24 weeks or 6 months, the agency will give the following deliverables to NI.
- Timeline to complete the assessment.
- A note on the Ethical considerations & adhere to it.
- Confidentiality of respondents to be maintained.
- Behavior Change Communication module on DFS & anemia.
- Local food frequency calendar for all the districts as a tool for the community & staffs.
- Local translation of research tools for pre-testing & standardization exercises.
- Anemia referral forms to block & district level public systems.
- Plan for training of interviewers & supervisors.
- Field procedure manual in English & Hindi languages.
- Clean & label data sets in the used software.
- Data analysis & findings of the post intervention study.
- Report of the Post Intervention study.
- Power point presentation summarizing the findings of the post intervention.
- Draft preparation for a peer reviewed journal based on literature review & analysis using inferential statistics.
- Findings of the post intervention to be disseminated in a meeting with NI.
- A final brief summary report & a full report.
- Final report in hard & soft copies.
- Research brief for dissemination.
- Publication in journals with multi authored articles.
OUTLINE OF THE BCC MODULE
The BCC or the Behavior Change Intervention module’s first section will deal with understanding the concept of behavior & related words. These are the words like behavior, habit, attitude, perception, thought & sustained activity.
The second section will lead with an intricate mechanism that we all go through while adopting a behavior. In this case, it is the regular use of DFS by consumers on a daily basis with a target to reduce prevalence of anemia.
Each one of us has prior information. In this case, it is the regular use of iodized salt. Now, the BPL families learn about the DFS. With this, they become aware about the DFS. As they become aware, they start accepting information about DFS. After acceptance, they try to find a meaning to the new behavior. When they seek a meaning, they get motivated. After finding a meaning, they put an effort to use the DFS. When they put an effort, they are actually weighing the pros & cons of using DFS. After this effort, they decide to apply or do the activity with support from others. After this decision, they use DFS on a day to day basis. When it becomes a daily activity, they start praising DFS & tell about the benefits to others. When they keep sharing the benefits with others, the use of DFS becomes a sustained activity for that mother & gradually other members of the family follow suit.
To demonstrate this, role play outlines will be given in the module so that the participants get an understanding of all the modalities of BCT.
DISSEMINATION
The post intervention study findings will be published not in academic journals but also in newspapers through short journalistic articles. This approach will address both the stakeholders of general population & academicians. Certification from the academic fraternity for the success of the pilot interventions will help the general population to up take the use of DFS. Dissemination will also be done in seminars & symposiums at various levels to increase awareness among masses.
Besides the print media, the audio-visual media & the social network platforms will also be used to disseminate the findings of the pilot & the current post intervention.
SUMMARY OF THE SCOPE OF WORK OF THE STUDY
- The study is for 24 weeks on the post interventions of a project that has been implemented.
- The base line & end line of the project used an experimental design to prove the efficacy of DFS on anemic individuals who are from BPL family.
- The post intervention study focuses on a Behavior Change Intervention strategy.
- The post intervention study uses a mixed method where both qualitative & quantitative approaches are used.
- Trainings or orientations are to held only after the development of modules.
CONCLUSION
The assessment process includes all the modalities that should go into the technical proposal while submitting the proposal for approval by an agency. The outline will be helpful for any stakeholder to develop a proposal & subsequently submit the proposal on any issue that they intend to work with.
The Research Methodology section will be helpful to the stakeholders while designing a research primarily to collect qualitative data. There is however a section on the quantitative data aspect through the In-Depth Interview Schedule that is proposed to be used for collecting data from the respondents.
The primary task of this proposed study is to make the base of the proposal on the lines of a Behavior Change Intervention to assess the effectiveness of a food fortification strategy to deal with the perennial challenge of anemia.
ACKNOWLEDGEMENT
Professor Shankar Das, the current Vice Chancellor of TISS, Mumbai was the Ph.D. guide of the lead author at TISS during 2011-2018. Professor D.P. Singh of TISS, Mumbai was the teacher of the lead author at TISS, Mumbai during 1995-1997. The lead author acknowledges the contribution of all the co-authors in the article.
CONFLICT OF INTEREST
There is no conflict of interest in the article.
FUNDING
There was no funding received for the article.
- Tripathy T, Das S, Tripathy A, Prusty U, Nayak C, et al. (2023) Homoeopathy in Nutritional Issues Induced by COVID 19 Crisis & Beyond. Int J Sci Res 12(04): 2277-8179.
- Kapil U, Kapil R, Gupta A (2019) National Iron Plus Initiative: Current Status and Future Strategy. Indian J Med Res 150(3): 239-247.
- Chand R, Suri Y (2024) Multi-Dimensional Poverty in India since 2005-06, A discussion paper, NITI Aayog, UNDP.
- Gupta N, Kochar G (2009) Pervasiveness of Anemia in Adolescent Girls of Low Socio-Economic Group of the District of Kurukshetra (Haryana). Internet J Nutr Wellness 7(1): 1-5.
- Kapil U, Kapil R, Gupta A (2003) Prevention and Control of Iron Deficiency Anemia Amongst Young Children and Adolescents: Theory and Practice in India. Indian J Pediatr 40(4): 293-295.
- Dandekar VM, Rath N (1971) ‘Poverty in India’, Economic and Political Weekly 6(1 & 2). pp: 25-27+29-48.
- Roy SS, Weide RVD (2022) Poverty in India has Declined Over the Last Decade but not as much as Previously Thought. Policy Research Working paper, 9994, World Bank, Washington DC.
- GOI, Anemia Mukt Bharat Dashboard. Available online at: https://anemiamuktbharat.info
- GOI, MOHFW, IIPS, NFHS 5 fact for India (2021).
- GOI, MOH, RGI, Census (2011).
- Wikipedia, www.wikipedia.com
- GOI, MORD, Aspirational Districts Program (2014).
- mapsofindia.com
- Singh M, Saini S Conceptual Review of Preventive & Social Medicine, second edition 2019-2020, CBS publishers & distributors Pvt Ltd, ISBN-978-93-88725-84-2.
- CNNS, 2016-2018, https://www.nhm.gov.in
-
 Table 1
Table 1 -
Table 2
-
Table 3





QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advances in Nanomedicine and Nanotechnology Research (ISSN: 2688-5476)
- Journal of Womens Health and Safety Research (ISSN:2577-1388)
- Journal of Agriculture and Forest Meteorology Research (ISSN:2642-0449)
- Journal of Genetics and Cell Biology (ISSN:2639-3360)
- Journal of Astronomy and Space Research
- Journal of Veterinary and Marine Sciences (ISSN: 2689-7830)
- Journal of Microbiology and Microbial Infections (ISSN: 2689-7660)


