1831
Views & Citations831
Likes & Shares
India being the most populous country in the world, there is still a lack of health infrastructure in the country. Having handled patients on a daily basis, providing daily nursing care, thus nurses are the main factor in transmission of HAI’s among the patient and HCW’s [3,4].
Many studies have been done on international grounds to assess the knowledge and awareness of HCWs in infection control and waste management [5,6]. In addition to education and training, CDC also suggests timely update and assessment for all HCWs in preventing the HAIs [7]. These educational programmes should be done on a regular basis for all HCWs dealing in patient care services in healthcare setup.
Although there have been various studies conducted in western world, this study paper is one of the first to be conducted in the Indian subcontinent. This study paper will also impart knowledge to all its readers, and also help the policy makers for setting up an effective curriculum in healthcare provider courses and proper management of training and research programs in IC in future.
METHODOLOGY
The study was done in a tertiary care corporate hospital in New Delhi.
Inclusion criteria:
- All HCWs working in the ICU of our hospital
Exclusion criteria:
- People not willing participation / filling questionnaire for the study
The study questionnaire is developed after detailed review of studies done in similar settings [2-4]. All the data was collected from healthcare workers. A structured questionnaire was made and given to participants for recording their responses online or in person. Responses were recorded as “true or false”.
Study Questionnaire used:
PART-I (Basic details):
- Name (optional)
- Gender (Male/Female)
- Work experience: fresher, 1 year, 1-3 years, 3-5 years, >5 years
- Workplace (ICU type): Medical / Surgical / Cardiac care / Pediatric
PART-II (Questions) Response - True / False:
- Nosocomial infections are infections spread by air, water and environment.
- Invasive procedures increase the risk of nosocomial infection.
- “Standard Precautions” in infection control applies only to healthcare workers.
- A total of 10 steps are followed in medical hand washing.
- Hand hygiene should be practiced if touching the patient surrounding.
- 1% sodium hypochlorite is used for cleaning of spillage of biomedical waste.
- A bag of Haemocoel is disposed of in a red color-coded bag.
- Human waste is disposed in black color-coded bags.
- Re-capping should be done for ABG syringes after the sample is taken out.
- Pulmonary TB patients with already completed 2 months of initial treatment are placed in an isolation room.
- Initial urine sample is the best for sampling and isolating organisms.
- Average amount of hospital waste generated per bed per day in an Indian government hospital is around 0.5kg-4kg.
- Cytotoxic drugs and expired medications are disposed of by autoclave.
- HCV is the most dreaded blood borne infection healthcare workers should be aware of, followed by HIV.
- Disinfectants kill microbes and spores present on the surface.
- Linen for in-patients must be changed every 4 h, regardless of being soiled or not.
- “Donning” is the process of wearing personal protective equipment.
- Gloves are the first to be removed in the “doffing” process.
- The time for hand washing (as per recommendation by WHO) is 2 min.
- After accidental contact with blood from a patient on a naked hand, the healthcare professional must go for a hand rub.
- Hand washing in running water is the first important step after a needle stick injury.
- Pus culture from the bedsore is taken from the center of the wound.
- Mycobacterium leprosy has the risk of spreading by touching the patient.
- Forceps used in daily activity must be thrown after single use.
- Blood contaminated cloth from HIV patient must be sent to incineration for sterilization
RESULTS
A total of 100 (n = 100) participants were enrolled for this study through online media.
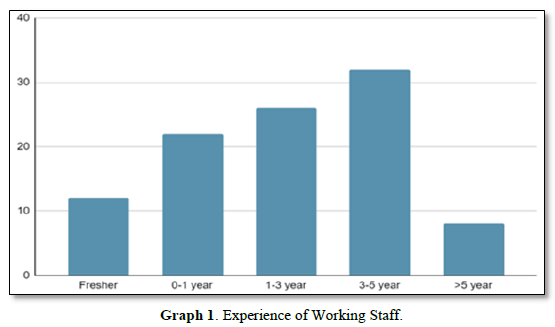
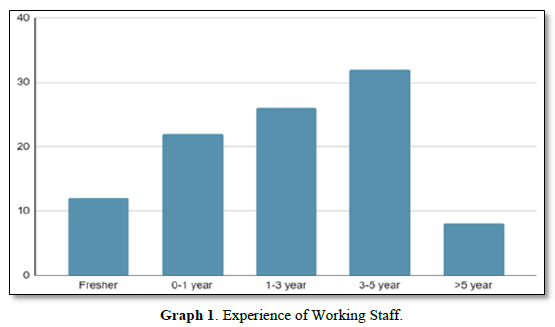
Majority of the staff working in the intensive care units (ICU’s) were having experience of 3-5 years (Graph 1).
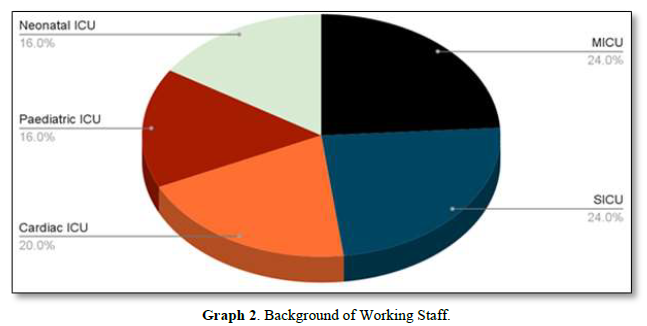
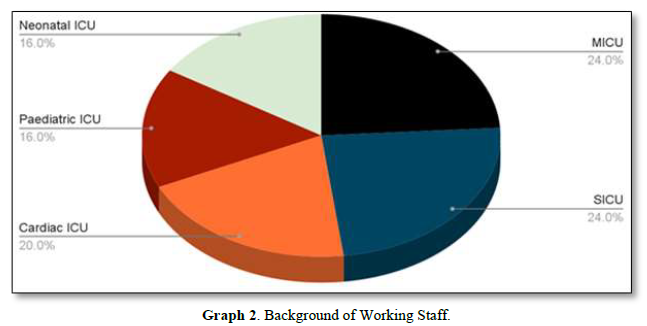
- Staff participating in the study are shown in the distribution (Graph 2 pie chart). Majority of the staff were from medical and surgical ICU.
- Majority of the staff participated were females (78) and males (22).
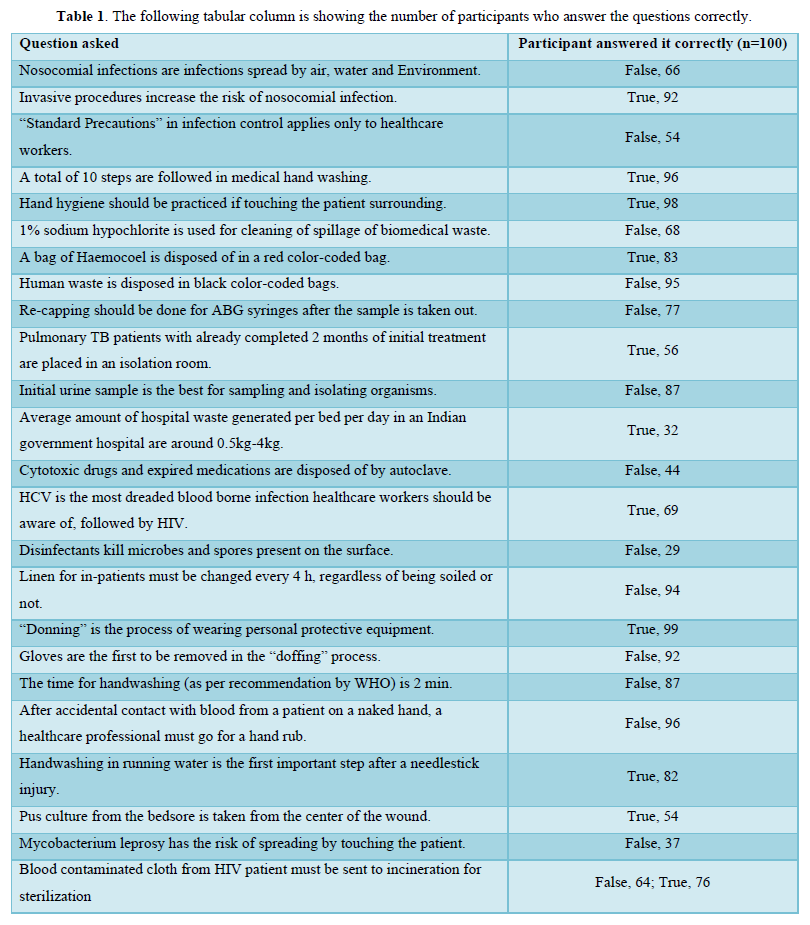
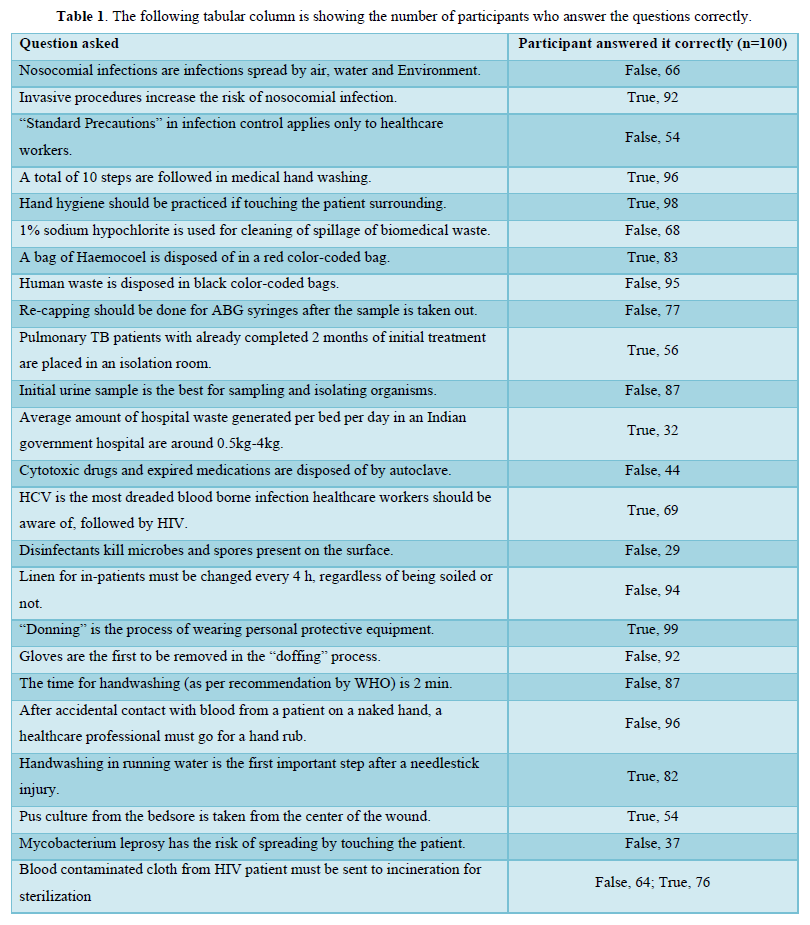
The following tabular column is showing the number of participants who answer the questions correctly (Table 1).
Majority of the correct answers were from Medical ICU, Pediatric and neonatal ICU. Theoretical knowledge was strong among pediatric and neonatal ICU. The staff, who participated in the study were correlated with their class attendance, and found that those who attended the classes and bedside learning in ICU’s were more accurate in answering correctly than those who didn’t attend the class.
Freshers, who were newly graduated and preparing for higher exams were having more accurate knowledge and a strong theoretical base, whereas, those with more practical based learning had more accurate skill learning in this study.
DISCUSSION
The current study was performed in a tertiary care hospital, aiming to assess the knowledge and awareness of nurses in infection control and biomedical waste management in high risk areas of the hospital, the intensive care unit (ICU). The nursing team demonstrated an overall acceptable awareness and knowledge about the infection control and biomedical waste management.
Around 83% of all the nurses in this study were consistent in attending the IC classes conducted in the hospital at regular intervals. Highest scores were achieved by nursing staff working in the medical ICU’s, pediatric and neonatal ICU, in contrast to our expectation as the nursing team recruited in the neonatal and pediatric ICU were majorly freshers and nurses with 1-3 years of experience. The surgical ICU and cardiovascular ICU nurses scores were above average but not satisfactory. The study highlights that the nurses had satisfactory knowledge about the safe disposition of biomedical waste (with >80% of all nursing recruits for the study answering the questions correctly). The study shows that participants in this study had less adequate theoretical knowledge, showcasing the need for more aggressive education in hospital setup, emphasizing theoretical inputs and practicing it in real life.
The study has shown that the nursing participants had excellent knowledge regarding hand hygiene and hand washing, use of hand rub, as per recommendation from the CDC and WHO [1,8]. This can be explained by rigorous regular training, continuous awareness and daily bedside inspection of the nursing team by IC nurses and in-charge (Figure 1).
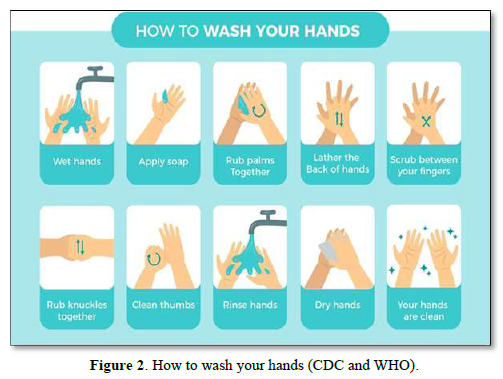
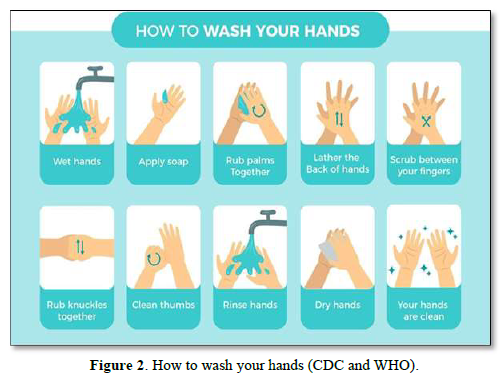
The correct mechanism of handwashing is shown in the image beside as per recommendation by CDC and WHO [1,8]. Hand washing is the most effective, affordable and simple method of preventing infection spread in the hospital and household setting [9].
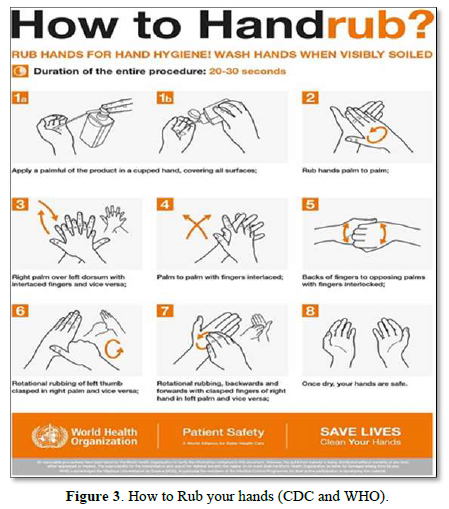
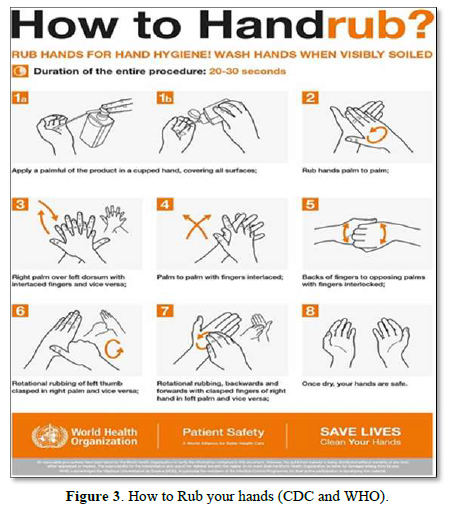
Hand rub is another method of preventing cross-spread of infection within the hospital compound. The hand rub should be done when [1,8,9] (Figure 2):
- Before touching the patient
- After touching the patient
- Before any procedure
- After any procedure
- Touching the patient surrounding
Hand rub should be considered always while handling patients, whereas handwash should be considered when the hands are visibly soiled [1] (Figure 3).
The study also showed that senior nurses (experience >3 years) and surgical ICU nurses had better knowledge of handling biomedical wastes and proper disposition of these biomedical wastes when compared to other nurses recruited in the study. This can be because of the knowledge gained over the years and day-to-day activity carried out in these ICU by the senior nurses.
The study has also shown the deficiency in theoretical knowledge among the nursing participants in the study. Only around 25% of all the participants had proper knowledge about the disease process, disease condition (theory taught during the nursing curriculum). The participants, who had correctly answered the theoretical questions were freshers, who had recently graduated from university. A further enquiry with these participants has shown that these participants were preparing for higher education and higher examination, thus, helping in overall enhancing their theoretical knowledge in IC.
There are variable results in this study, and, this study is limited due to its fewer participants in this study. This study only included nurses from ICU’s, leaving behind nurses of wards and emergency room and OPD. Thus, this study is limited and we need a proper multicenter study to evaluate all the HCW’s for IC and BMW management.
CONCLUSION
The study conducted by us in a tertiary care center of Delhi, North India, involved the majority of the healthcare workers (i.e. ... nurses) working in the ICU’s. The study has shown that participants are aware of the IC and BMW management. Experience in this field played an important role in assessing the skill and awareness among the participants. Proper bedside teaching, regular lectures and hand-on training, based on the guidelines set by CDC and WHO, played a vital role in proper enhancement of knowledge and awareness among HCWs regarding IC and BMW management. This study concludes that regular training, bedside teaching from time-to-time is necessary for better IC and BMW management among the HCW’s. A more detailed multicenter study is required for better assessment and analysis of HCW’s for IC and BMW management.
- World Health Organization (2015). Health care‐associated infections FACT SHEET.
- Wu CJ, Gardner GE, Chang AM (2008) Taiwanese nursing students' knowledge, application and confidence with standard and additional precautions in infection control. J Clin Nurs 18: 1105-1112.
- Colet PC, Cruz JP, Alotaibi KA, Colet MKA, Islam SMS (2017) Compliance with standard precautions among baccalaureate nursing students in a Saudi university: A self‐report study. J Infect Public Health 10: 421-430.
- Valim MD, Marziale MHP, Richart‐Martínez M, Sanjuan‐Quiles Á (2013) Instruments for evaluating compliance with infection control practices and factors that affect it: An integrative review. J Clin Nurs 23: 1-18.
- Tavolacci MP, Ladner J, Bailly L, Merle V, Pitrou I, et al. (2008) Prevention of nosocomial infection and standard precautions: Knowledge and source of information among healthcare students. Infect Control Hospital Epidemiol 29: 642-647.
- D'Alessandro D, Agodi A, Auxilia F, Brusaferro S, Calligaris L, et al. (2013) Prevention of healthcare associated infections: Medical and nursing students' knowledge in Italy. Nurse Educ Today 34: 191-195.
- AL‐Rawajfah OM, Tubaishat A (2017) A concealed observational study of infection control and safe injection practices in Jordanian governmental hospitals. Am J Infect Control 45: 1127-1132.
- Center for Disease Control and Prevention (2007) 2007 Guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings.
- El‐Gilany AH, Badawy K, Sarraf B (2012) Knowledge of health care providers of standard precautions and infection control at students' hospital, Mansoura University, Egypt. TAF Prevent Med Bull 11: 1-6.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Diabetes (ISSN: 2644-3031)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Pathology and Toxicology Research
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)