Review Article
Recent Advances in Phytoleads for Management of Respiratory Disorders
2789
Views & Citations1789
Likes & Shares
Respiratory disorder is one of the common disorders that is related with Respiratory Track. Respiratory disorders continue to be a major health challenge worldwide especially due to the increasingly fast development of resistance to the drugs currently in use. Many Phytoleads or Phytoconstituents are traditionally used for respiratory illness treatment, and some have been investigated for their efficacy with positive results. In this review, all the phytoleads or phytoconstituents having anti-inflammatory activity and some of them possess antioxidant activity too. All are used to treat respiratory tract inflammation. Curcumin used as antiasthamatic also. The results of this study show that phytoleads or phytoconstituents are used for the treatment of respiratory system disorders. The information gained on frequently used phytoleads might give some leads for future targets for further analysis in order to develop new drugs.
Keywords: Respiratory diseases, Phytoleads, Isolated compound, NDDS for Phytoleads, Covid-19
INTRODUCTION
Lung diseases are one of the leading causes of death globally. It is characterized by airflow limitation, loss of elasticity, chronic inflammation, emphysema, bronchoconstriction and mucus hyper secretion. Several factors including genetics, tobacco smoke, air pollution, inhalation of noxious particles, occupational chemicals and dusts have shown to contribute to the development of lung disease. Some of the most widespread are asthma, chronic obstructive pulmonary disease (COPD), occupational lung diseases and pulmonary hypertension. Some disorders are moderate to lethal and life threatening like tuberculosis and pneumonia [1].
ANGIOGENESIS RELATED DISORDERS IN LUNGS
Angiogenesis is the growth of new capillary blood vessels in the body. It is an important natural process for healing of wound and redevelopment of new tissue. The body has ability to control angiogenesis by producing a precise balance between growth and inhibitory factors during neovascularization. When imbalance is occurred, it leads to the development of less or a greater number of blood vessels [2,3].
Various disorders have excessive angiogenesis as an underlying mechanism. Abnormal blood vessel growth, either excessive or insufficient is responsible for the development of deadly conditions like cancer, skin diseases, diabetes, cardiovascular diseases, stroke, age-related blindness and lung disorders [4].
Low immune functioning, adverse climatic conditions, intolerable air pollution, excessive exposure to smoke and other toxic materials and presence of fungal, viral, bacterial infections are some common causes of lung disorders. Lungs are characterized by double vascularization, first is bronchial vasculature, associated with thoracic aorta and second is the pulmonary system which is part of the air/blood barrier of the lung tissue [5].
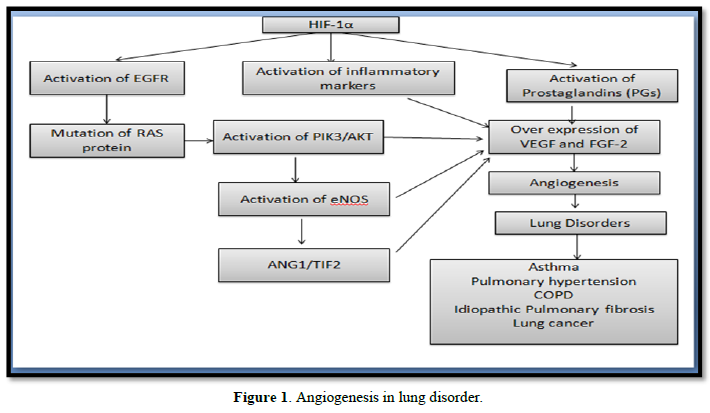
Lung tissue produces VEGF and FGF-2 which is an important growth factor necessary for building of lung tissue architecture. Exposure of lung tissue to intolerable air pollutants, excessive smoke and other toxic gases triggers overexpression of VEGF and FGF-2 in lung tissue architecture by activation of inflammatory flood which is an important reason for the development of abnormal angiogenesis in lung and later causes development of lung cancer [6].
COPD is associated with significantly reduced capillary length density and hypoxia condition followed by activation of HIF-1α which plays an important role in the development of angiogenesis [7].
Whereas, asthma is associated with airway congestion and re-modulation because of the development of inflammation and deposition of mucus plug in respiratory tract which is linked with excessive angiogenesis [8]. Cytokines, cell adhesion molecules, growth factors, vasoactive peptides, proteolytic enzymes (metalloproteinases) and plasminogen activators play a vital role in the development of above-mentioned condition which activates EGFR/PI3K/AKT/mTOR pathways. Activation of these pathways is responsible for the activation of endothelial growth regulator followed by overexpression of VEGF and FGF-2 [3]. Lung disorders like asthma, COPD, Idiopathic pulmonary fibrosis and pulmonary hypertension develop edema, inflammation, fibrosis, airway obstruction, decrease ventilation and damage to alveolar capillaries. These conditions are responsible for the inadequate supply of oxygen to the lung tissue. If an insufficient supply of oxygen continues for a long time, supplementary mechanisms attempt to restore oxygenation or help the body adapt to hypoxia. Hypoxia is mediated by hypoxia-inducible factors (HIFs) having 2 subunits HIF-1α/2α and 1β [9]. Decreased oxygen supply after a period stabilizes HIF-1α through post-translational modification. Once it stabilizes, α subunit is cleaved off and binds to the β subunit this hetero dimer then binds to numerous promoters containing hypoxia response elements (HREs), leading to the transcription target genes of VEGF. Hypoxia-inducible factor (HIF-1) activates epidermal growth factor (EGF) which causes over expression of VEGF in lung tissue. Nitric oxide synthesis is regulated by the enzyme NO synthase specially eNOS/NOS3 isoform. This isoform plays a key role in VEGF-induced angiogenesis which is obtained by phosphorylation of eNOS isoform at serine 1117 residue by AKT or by hypoxia [10]. Uncontrolled inflammation is the main factor behind the pathogenesis of various lung disorders. Inflammation leads to alterations in the bronchial epithelium and lung micro environment [11].
Various pro inflammatory markers like transforming growth factor-beta (TGF-β), platelet-derived growth factor (PDGF), interleukin 6 (IL-6), interleukin 8(IL-8) which activates signal transduction and activator of transcription 3(STAT3) pathway. Subsequent STAT3 phosphorylation is involved in upregulation of angiogenic mediators, such as VEGF, FGF-2 and HIF1 which leads to angiogenesis [12].
Beside this Cyclooxygenase (COX)-2, an inducible enzyme that catalyzes the formation of prostaglandins (PGs) from arachidonic acid in lung tissue, is also activated by hypoxia and it helps in the stimulation of VEGF gene expression [13].
Oxidative stress in asthma and COPD is associated with airway inflammation by activating inflammatory gene expression. The nuclear factor-kappaβ (NF-κβ) is an important factor that regulates cytokine activity in the airway during inflammation [14] (Figure 1).
Asthma
It is a chronic respiratory disease in the airway characterized by episodes of wheezing, shortness of breath, coughing and chest pain. The common elicit of asthma such as airway irritants like tobacco smoke, air pollution, allergens, respiratory infections, stress, mold and termites and it is caused through genetic and environmental factors also the asthma attack begins, when the allergen inhaled through respiration and it binds to the IgE antibodies on mast cell in the lung and the mast cell produced histamine, leukotrienes. These biologically active mediators cause the smooth muscle cells or bronchial contract. This cause narrowing the lumen of the bronchi due to the accumulation of eosinophils. The repeated attacks or accumulation of eosinophils causes bronchial damage in the lung. In the late stage of the asthma attacks is difficult to breathing due to the smooth muscle cells in the bronchi constrict, and the airway become inflamed and swollen. Asthma is typified by airway eosinophilia, edema, mucus hypersecretion, bronchial epithelial injury and hyperactivity. Disease pathogenesis includes contributions from several cell types including airway epithelial cells, eosinophils, macrophages, dendritic cells, T-helper type 2 (Th2) cells, IgE-secreting B cells and mast cells, as well as changes in broncho alveolar lavage fluid [15].
COPD
The pathological factors affecting COPD are diverse and intricately linked. In the deteriorating progress of COPD, various inflammatory mediators are released from epithelial cells and infiltrated inflammatory cells in the lungs, including neutrophils, macrophages and T lymphocytes. It is important that pro inflammatory cytokines such as tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1) and IL-6 and chemokines including IL-8 activate and attract the circulating cells in the pathological process. Transforming growth factor-β (TGF-β) has been reported to cause airway fibrosis, leading to airway destruction. Several approaches for blocking these cytokines and few among them, IL-1β and IL-18, key molecules of inflammasome, are suggested as potential targets along with other inflammasome components [17].
Reactive oxygen species (ROS) are also critical for provoking COPD. Tobacco smoke contains high concentrations of oxidants and induces a variety of free radicals including ROS which amplifies the inflammatory responses and develops the pathological stage of COPD. Therefore, several molecules linked to oxidative stress, such as nuclear erythroid-2-related factor 2 (Nrf2), NADPH oxidase, myeloperoxidase and superoxide dismutase may be considered targets for COPD therapy. Especially, matrix metalloproteinase (MMP) and neutrophil elastase are intricately regulated in COPD pathology. Several reports indicate that the activation and/or elevated expression of matrix metalloproteinases such as MMP-2, -9 and -12 are closely related to the development of COPD [19].
Recently sirtuins were demonstrated to be deeply involved in COPD. The level of sirtuin 1 expression is reduced in the lungs of COPD patients. The activation of sirtuin 1 and 6 has been shown to have protective effects against COPD [20] and sirtuin activators may be proposed as candidates for COPD treatment. Leukotriene B4 (LTB4) and prostaglandin E2 (PGE2) levels in the exhaled breath condensate of patients with COPD are higher than in healthy subjects [22]. LTB4 is a potent neutrophil chemoattractant and its concentration in sputum is also increased in COPD patients [21]. To reduce LTB4 levels, antagonists of LTB4 receptors and 5-lipoxygenase inhibitors have been developed for the treatment of COPD. Inducible nitric oxide synthase (iNOS) is widely up-regulated in the airways and peripheral lungs of COPD patients [23]. NO synthesized by iNOS and its oxidant peroxynitrite cause oxidative stress in the lungs. In the animal model, iNOS inhibition by a selective inhibitor was shown to partially improve pulmonary vessel remodeling and functional destruction by smoke-induced emphysema [24]. Recent investigations suggested that interrupting signal transduction pathways may alleviate COPD progress. Various kinases participate in regulating the expression of inflammatory genes and transcription factors related to COPD. The p38 mitogen-activated protein kinase (MAPK) and phosphoinositide 3-kinase (PI3K) are proposed as promising representative targets for the development of selective inhibitors. The activation of p38 MAPK induces inflammatory mediators such as IL-1β, IL-8 and MMP in various inflammatory cells, leading to the exacerbation of COPD symptoms. The inhibition of p38 MAPK showed efficacy in a six-month clinical trial in COPD patients with ≤2% blood eosinophils [25].
PI3K-mediated signaling in macrophages and neutrophils is involved in inflammation and immune responses and the activity is up-regulated in the lungs of COPD. It was found that blocking certain isoforms of PI3K reduced pulmonary neutrophilia in a murine smoke model [26].
Several PI3K inhibitors have been developed as candidates for COPD therapy so far. In addition, inhibitors targeting transcription factor, nuclear transcription factor-κB (NF-κB), which is involved in the encoding of many inflammatory genes and relevant kinases such as IκB kinase have been also investigated [27].
Pneumonia
Pneumonia is a respiratory tract infection characterized by the inflammation of one or both lungs as a result of the accumulation of pus in the alveoli. Pneumonia which can be caused by bacteria, viruses or fungi can be mild, severe or life threatening. Bacterial pneumonia can be caused by Streptococcus pneumoniae which is the commonest cause, Staphylococcus aureus, Moraxella catarrhalis, Klebsiella pneumoniae, Hemophilus influenza, Chlamydophila pneumonia and Legionella pneumophila. Pneumocystis jirovecii pneumonia (PCP) is a fungal pneumonia commonly found in immunocompromised patients. Viral pneumonia can also be caused by adenovirus, Varicella zoster, Influenza virus and respiratory syncytial virus [28,29].
Tuberculosis
Tuberculosis (TB) is an airborne infectious disease which does not only affect the lungs but also other parts of the body such as the brain and spine. The main cause of TB is Mycobacterium tuberculosis. Other M. tuberculosis complex that causes TB include M. bovis, M. africanum, M. canetti and M. microti. The predominant symptoms of active TB are fever, night sweat, weight loss and chronic cough with blood containing sputum. Treatment of TB is very tedious and requires a long course with multiple antibiotics involved [30].
Pulmonary hypertension
Pulmonary hypertension (PAH) is a progressive disease associated with increased blood pressure between lung and heart through lungs which is responsible for increased pulmonary vascular resistance (PVR) and ultimately heart failure. Shortness of breath, chest pain and fainting episodes are common symptoms associated with PAH because of vascular remodeling produced by excessive cell proliferation and reduced rate of apoptosis. According to the World Health Organization, Pulmonary hypertension is classified depending upon following symptoms.
- Pulmonary arterial hypertension (PAH) is associated with increased pressure in the vessel caused by an obstruction in the small arteries in the lung
- Pulmonary hypertension because of left-sided heart disease
- Pulmonary hypertension because of hypoxia
- CTEPH (chronic thromboembolic pulmonary hypertension) -Blocking blood flow in the lung because of clot formation
- Pulmonary hypertension because of numerous potential metabolic, systemic, or hematologic conditions
Pulmonary arterial hypertension (PAH) is also characterized by an imbalance between angiogenic and anti-angiogenic factors which lead to lung vessel obliteration. PAH is widely considered a proangiogenic disease but the involvement of angiogenic factors, such as the VEGF and its receptors, in the pathobiology of PAH remains incompletely understood. In severe forms of PAH, the pulmonary vascular resistance is elevated because of pulmonary vasoconstriction, lung vessel remodeling, or both [2].
Idiopathic pulmonary fibrosis
Idiopathic pulmonary fibrosis (IPF) is a chronic disease characterized by fibrosis of the lung parenchyma. It is caused by repetitive alveolar epithelial cell injury and uncontrolled proliferation of lung fibroblasts. These fibroblasts exhibit unregulated proliferation which differentiates it into myofibroblasts associated extracellular matrix (ECM) proteins in the interstitial space. A number of profibrotic mediators including tumor necrosis factor-α, interleukin (IL)-1β, IL-13, transforming growth factor (TGF)-β, connective tissue growth factor (CTGF) platelet-derived growth factor (PDGF), VEGF and FGF-2 and their signaling cascades are believed to play a crucial role in the pathogenesis of IPF [2].
Lung cancer
Lung cancer is a life-threatening disease associated with the abnormal and unrestrained growth of lung cells. Lung cancer mainly starts from bronchi, it invades nearby tissue and spread throughout the body. There are mainly two types of lung cancer, small cell lung cancer (SCLC) which is more aggressive, quickly grown and widely spread in other organs. Non-small cell lung cancer (NSCLC) is a slow growing type of cancer. NSCLC is further classified into various types depending upon tissue where the tumor is developed. Adenocarcinoma (40% of NSCLCs), Squamous Cell Carcinoma (25-30% of NSCLCs), Large Cell Carcinoma (10-15% of NSCLCs) are the main type of NSCLC. Genetic abnormalities are also found in some past researches which have the main role in the development of NSCLC. Activation of EGFR and ALK gene arrangement are basic pathology involved in the progression of lung cancer. According to the report by Daniela Frezzetti and co-workers, it was found that VEGF is a potential target in lung cancer. Activation of EGFR signaling is highly linked with the activation of VEGF. VEGF block the tyrosine kinase activity with the consequent inhibition of multiple proangiogenic and proliferative signaling pathways. A clinical study by Masato Shingyoji also revealed that abnormal growth of lung cells in patient is because of the over-expression of VEGF. Various report on anti- VEGF therapy including endostar combined with cisplatin on the expression of VEGF lewis lung cancer rats [2].
WHY MEDICINAL PLANTS ARE BETTER CHOICE?
In present drug discovery era, a variety of chemically synthesized molecules are approved by regulatory bodies and are coming on the marketplace, having good therapeutic value but this therapy causes serious side effects which could be life threatening. Conventional therapy provides non-target ability in body due to peak and valley fluctuations of plasma drug concentration and a frequent dose of administration can produce troublesome for allopathic therapy led to poor patient compliance. Approximately 80% of the present world population relies on use of herbal medicines for their primary health care and other needs which denotes the scope of herbal medicines. Furthermore, herbal medicines own variety of therapeutic actions and are less-toxic with fewer adverse effects. Presently, herbal medicines have regained their reputation for treatment of lung diseases with their efficiency and safety feature being strongly supported by controlled clinical trials. Current global research has also presented valuable inputs about specific mechanism of action of these herbal alternatives [1].
Phytoconstituent or Phytoleads
Phytoconstituents are nothing but the chemical moieties that appears naturally in plants and which are responsible for various organoleptic and therapeutic features of plants. More specifically, these chemical moieties are secondary metabolites such as alkaloids, glycosides, polyphenolic compounds and etc. Phytoconstituents and their health-related consequences have been extensively scrutinized in this century. Their therapeutic outcomes are of main interest because of their role in prevention of major life-threatening diseases such as cancer, cardiovascular complications and respiratory infections. These diseases are leading causes of death nowadays which signifies that phytoconstituents will persist to be matter of scientific community interest. Based on practical health benefits such as anti-oxidant, anti-inflammatory and immuno-modulatory, phytoconstituents may act as a budding additive and/or an alternative therapy [1].
Phytoconstituents in inhalation delivery
It is an appealing to think of inhalation therapy as a novel approach for drug delivery. Main focus of scientists is trying to utilize this non-invasive therapy to treat various extrapulmonary diseases also. Lung, is persistently exposed to an environment rich in oxygen and thus prone to injury caused by oxidative stress. So as to impede lung tissue damage, lung is endowed with various antioxidant protections such as glutathione, superoxide dismutase, β-carotene, vitamins C and E, uric acid and heme-oxygenase. phytoconstituents such as flavonoids i.e., polyphenolic compounds are natural Antioxidant. anti-inflammatory and antibacterial activities of polyphenolic compounds are documented, antioxidant and anti-inflammatory compound in lung tissue distributing aerosol directly to airways by a nebulizer, a pressurized metered dose inhaler (pMDI), soft mist inhaler (SMI) or a dry powder inhaler (DPI)are used. DPIs can enhance phytoconstituent physicochemical and biopharmaceutical properties and can guarantee a delivery of higher drug concentration at the deposition site [1] (Table 1).
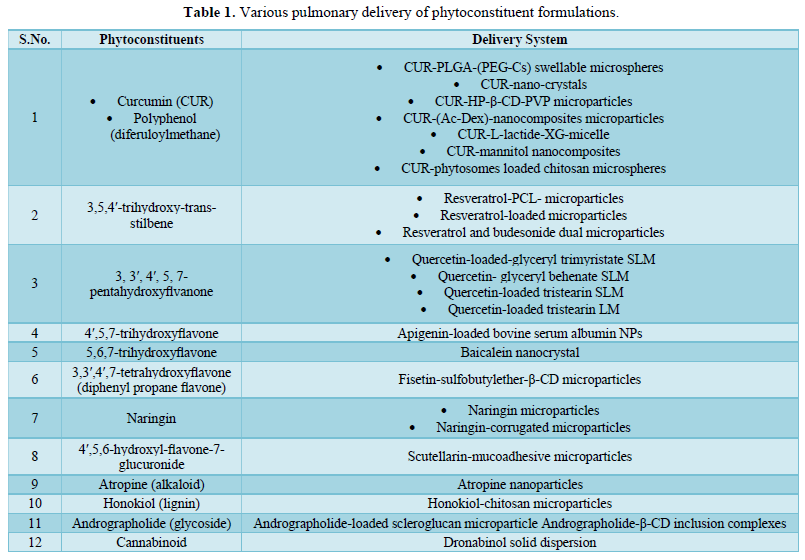
All the above phytoconstituents having anti-inflammatory activity and some of them possess antioxidant activity too. All are used to treat respiratory tract inflammation. Curcumin used as antiasthamatic (Table 2).
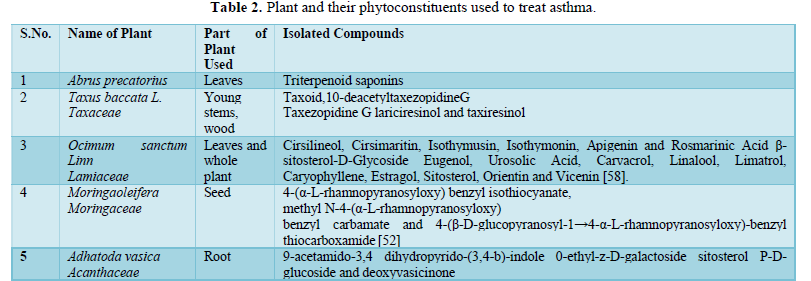
Till now many phytoconstituents were discovered for anti-asthmatic activity and several plants having these constituents to treat asthma related problems. These plants are: Curcuma longa, Aerva lanata, Cynodon dactylon, Piper betle, Lepidium sativum, Curculigo orchioides, Casuarina equisetifolia.
Medicinal plants with demonstrated activity against pneumonia:
- Echinops adenocaulos
- Verbascum fruticulosum
- Parietaria Judaica
- Urtica urens
- Beta vulgaris [30]
Medicinal plants with demonstrated anti-tuberculosis activity:
- Anogeissus leiocarpa
- Terminalia avicennioides
- Capparis brassii
- Combretum spp.
- Solanum torvum
- Galenia africana
- Allium sativum
- Allium cepa
- Cinnamomum verum
- Acalypha indica [30].
NDDS for Phytoleads: Phytoleads are to be incorporated in the suitable delivery agents for better and site-specific action or local action. Novel drug delivery system enhances bioavailability of particular molecule and act locally hence reduce adverse kind of effect. In allopathy system it is the most trending system of drug delivery. It is also used in phytopharmaceuticals for delivery. Phytosomes, liposomes, neosomes, ethosomes, nano particles, nano gel, and many more are used. “Phytosome Complexed with Chitosan for Gingerol delivery in the Treatment of Respiratory Infection” was already done Singh RP [40].
RECENT WORK IN PHYTOLEADS
Recent global pandemic COVID-19
Currently entire world is under the threat and suffering from the infectious disease known as COVID19. It is a very dangerous issue of health hence within a short time period many researches being processed and many literatures suggest the pathophysiology of this virus. It is major and largest single strand RNA virus damaging the respiratory system in humans. No therapeutic options available to cure the infection in till date which increases the mortality rate across the countries. India is a hub for traditional alternative system of medicine and therefore possibility to find solution to fight against COVID-19 is obviously possible amongst the sources. Although most of the corona virus infections are associated with mild clinical symptoms in human, main two beta corona viruses are responsible for two serious epidemics; severe acute respiratory syndrome corona virus (SARS-CoV) and middle east respiratory syndrome corona virus (MERS-CoV) in the world [41].
SARS-CoV-2 virus, is a serious infection of the respiratory tract which affects both the upper respiratory tract including throat, nose and sinuses and lower respiratory tract, i.e., windpipe and lungs, of a person.
Anatomy of COVID 19
Corona viruses are spherical enveloped positive sense RNA viruses from Coronaviridae family and order Nidovirales [43]. CoVs are the large genome size RNA viruses with sizes in the range of 26 to 32 kilo bases in length. Genome of CoVs encodes for four key structural proteins viz. i) spike (S) glycoprotein, iii) nucleocapsid (N) phosphoprotein, ii) membrane (M) glycoprotein, and iv) envelope (E) glycoprotein. In SARS-CoV-2 virus, hemagglutinin-esterase (HE) protein is also found in the virus envelope. All these proteins are vital for the development of complete virion structure. The S glycoprotein, which forms a homotrimer protruding from the virus surface, mediates the entry of the virus into the host cells. S protein has two functional subunits where S1 subunit is associated with the binding of the virus with the host cell angiotensin-converting enzyme 2 (ACE2) receptors and S2 subunit assists the fusion of the virus with the cellular membrane.
Pathophysiology of COVID 19
The virus is enveloped and single stranded positive RNA type of virus.The virus enters into host having characteristics receptors recognized by virus spike protein. After entry into the host cell there are 16 nonstructural proteins like RNA dependent RNA polymerase, non structural protein-12. This is vital for generating full length virus RNA.The non structural proteins have function like suppression mRNA of host cell which might be the role of suppress immune response of host. For COVID19 the receptor in human was identified as Angiotensin-Converting Enzyme 2. The pathogenesis suggests that virus affect ACE2 site. The effect of virus cause cells normal function to get disturbed. The enzyme is zinc containing enzyme working for cleaving angiotensin 2 into angiotensin 1, cleavage of bradykinin, dynorphin A and ghrelin. In case of considering the site of viral entry the cleavage function is disturbed for ACE2. This will lead to increase bradykinin. The literature also suggest bradykinin cause dry cough. Bradykinin is also known as chemical mediator causes increase capillary permeability and smooth muscle contraction, so it will cause edema in lungs and disturbed gas exchange function in alveoli [42].
Current management option
Oxygen supplementation, mechanical ventilation is currently major instrumental management measures.Currently, approaches like combination drugs containing lopinavir/ritonavir generally anti-retroviral drugs 400mg /100 mg every 12 h, chloroquine which is anti-malarial 500 mg every 12 h, hydroxychloroquine anti malarial 200 mg every 12 h. Alpha-interferon also a proposed approaches used [41].
Medicinal plants and their phytoconstituents used for prevention and cure of COVID19
Piper Nigrum L. (Black Pepper, Kaali Mirch): Extract having many pharmacological activities like antiviral, anti-bacterial, antiinflammatory, anti-pyretic, anti-oxidative, anti-thyroid, antitumor, immune modulator. its phytoconstituents can be used. Some of them phytoleads are Piperine, feroperine, piperylin, N-trans-feruloylpiperidine, piperoleine A, dehydropipernonaline, pipernonaline, pipertipine and they are used as antiviral agents [43].
Ocimum sanctum (Holy Basil, Tulsi): Its therapeutic potential as antibacterial, antidiabetic, anti-carcinogenic, anti-viral, anti-inflammatory, cardio-protective, immune system booster etc. [50] In Ayurveda, Tulsi is denoted as “Elixir of life” for its healing capability and promising potential in curing different health ailments including bronchitis, pyrexia, rheumatism, asthma, skin diseases, parasitic and microbial infections, gastric and hepatic disorders etc. Apigenin and Ursolic acid are found to be the main active antiviral ingredients in the Tulsi extract [42].
Nigella sativa (Black Cumin, Black seed, Kalonji): Thymoquinone is the main active phytochemicals present in black cumin and responsible for most of its therapeutic properties. Regarding its implication as antiviral properties, Nigella sativa oil and seeds have showed viricidal properties against various deadly viruses including hepatitis C virus (HCV) and HIV [53].
Cinchona officinalis (Cinchona, Quinine): Antiviral properties of chloroquine are explored against HIV and then against SARS-CoV-1, which has structural similarity to novel SARS-CoV-2. In clinical trials, chloroquine treated group is found to be superior in shortening the disease course, improving lung imaging findings, pneumonia exacerbation and increasing virus negative seroconversion with no side effects compared to control group. Dose- 500mg twice a day for 10 days [43].
Sambucus nigra (Elderberry): It boost immune system of the body [48].
Tinospora cordifolia (Giloy, Guduchi): It includesbiologically important phytochemicals including lactones, alkaloids, glycosides, steroids, sesquiterpenoid, diterpenoid, aliphatic compounds, phenolics, polysaccharides and flavonoid which play immunomodulatory activity inhuman body. It has anti-diabetic, antioxidant, anti-inflammatory, antiperiodic, antispasmodic, anti-arthritic, anti-allergic, antimicrobial, anti-osteoporotic, antitoxic, anti-stress, anticancer, anti-HIV, wound healing, cardio tonic, carminative, bitter tonic, blood purifier properties. Methanol extract of Giloy is found to have broad spectrum antimicrobial effectiveness against various strains which are Staphylococcus aureus, Klebsiella pneumonia, Escherichia coli, Shigella flexneri, Salmonella paratyphi, Salmonella typhimurium, Salmonella typhi, Enterobacter aerogene, Pseudomonas aeruginosa, Serratia marcesenses and Proteus vulgaris. Due to its alkaloid components including tinosporin, tetrahydropalmatine, choline, palmatine and magnoflorine, it also has protective role against aflatoxininduced nephrotoxicity [43].
Giloy (Size on one Bhibdi) + Tulsi (6 leaves) + Ginger (1/2 tsp.) + Kali mirch (4-6 seeds) Crush/Grind them all together and use it as herbal tea or mix it with honey and consume it. It can control cough, fever and also support immunity. Giloy juice hould be administered orally.
Azadirachta indica (Margosa, Neem): It is having various pharmacological activities. The whole plant is full of therapeutic value. Various extract and isolated constituents are used for numerous activities. Aqueous neem leaf extract is reported to have remarkable antiviral activity against measles virus, Chikungunya and Vaccinia virus [43].
Syzygium aromaticum (Clove): It is a rich source of phenolic constituents like eugenol, thymol, eugenol acetate, and gallic acid and also βcariophyllene and have enormous potential for cosmetic, pharmaceutical, food and agricultural applications. It has analgesic, antioxidant, antitumor, antiviral, antifungal, antiinflammatory and antibacterial activity. Eugeniin phytochemical is revealed to have good antiviral activity.Eugeniin reveals antiviral properties by inhibiting the virus DNA polymerase enzyme and subsequently prohibiting the DNA synthesis [44].
Pranax ginseng: The major chemical compositions of ginseng are triterpenoid, protopanaxadiols, protopanaxatriols and steroidal saponins also known as ginsenoid, polysaccharides and proteins which are responsible for their potential activities against antibacterial or like other activity especially for pathogens that cause respiratory infections in human body.The antiviral activity of ginseng is due to its efficiency to block viralattachment, membrane penetration and inhabiting virus replication inside the host cell [45].
Glycyrrhiza glabra (Liquorice, Licorice): The pharmacologic perspective of glycyrrhizin-a triterpene saponine, which can be a potential phytochemical against COVID-19. The study reports about the binding of angiotensin and converting enzyme II (ACE2), also down-regulating pro-inflammatory cytokines and also blocking the inhibition of accumulation of intracellular ROS, thrombin, hyperproduction of airway exudates and inducing endogenous interferon.Glycyrrhizic acid (GL) inhibited Epstein–Barr virus (EBV) replication with an IC50 value of 0.004 mM by inhibiting viral DNA polymerase GL showed antiviral activity against SARS-CoVs in Vero cells with a SI of 67 by reducing replication and inhibiting penetration and adsorption of the virus [59].
Andrographis paniculatais (Kalmegh): Recently investigated the inhibitory role of Androgra pholideas against SARS-CoV-2 proteases using an in-silico methodology [60].
Allium sativum (Garlic): The antiviral property may be helpful in reducing the severity of colds, flu or COVID-19 infection. Hence, Garlic boosts the immune system and helps in fighting against viruses and other diseases. It has Allicin which is board spectrum antibiotics [61]. It is reported to enhance immune health by stimulating protective white blood cells like NK cells and macrophages [62].
Zingiber officinalis (Ginger): It is having phytoconstituent such as Zingerone, 6-Gingerol, Paradol, Phellandrene, Zingiberene, 6-shagaol. Ginger is having powerful immune boosting property with addition of antiviral properties [43].
Piper betel (Betel vine): It is having immunity boosting activity [48].
Curcuma domestica (Turmeric): The main phytochemical includes diarylheptanoids such as curcumin, demehoxycurcumin and bisdemethoxycurcumin, germacrone, turmerone, atlantone and zingiberene are the group of major essential oils which are present in turmeric. Due to its antiviral effect the domestic sales of turmeric have also increases. Turmeric helps in the natural cleansing of the respiratory tract; it also supports in fighting against infection and its anti-inflammatory quality relieves individuals in cases of cold and flu. It is well known fact that the lower immunity is a risk in its own way and Curcumin is very helpful in addressing such issues and enhancing the immunity system. Curcumin inhibits inflammation, relieves congestion and pain thereby supports in improving the breathing process of patients with bronchial problems like sinusitis, sinus during respiration. The main upper respiratory tract problems include congestion, cough, bronchial asthma, cold and shortness of breathing andthus affecting children and elderly population. Due to inflammation of the air ways, the process of breathing becomes difficult [43].
Withania somnifera (Ashwagandha, Indian ginseng): Whithanone reduces the electrostatic component of binding free energies of ACE2-RBD complex and thus block or weakens the COVID-19 entry and its subsequent infectivity. It is also reported that the host cells namely ACE 2 in the human body got entrapped by SARS-CoV-2 with the help of its spike protein Receptor-Binding Domain (RBD). Ashwagandha could be the top choice among various medicinal herbs in this prospective fight against COVID-19 infectivity. Ashwagandha roots have high antiviral activities.
Pineapple/ Ananas comosus: Bromelain is a general name for a family of sulfhydryl proteolytic enzymes obtained from stem or fruit. Bromelain possess antiplatelet and anti inflammatory activity as well as it also possess activity to decrease substance P and edema. Bromelain also have tendency to decrease bradykinin. Bromelain is also potent anticancer and immunomodulators [42].
Haritaki/ Terminelia Chebula: Haritaki have proven anti-histaminic activity. Haritaki also possess cardio protection by lysosomal membrane stabilization activity, antiviral activity,Its phenolic content potential to inhibit sialic acid might be source to consider for anti viral activity [55].
Other medicinial plant can be used: Eucalyptus flowers (Eucalyptus globulus Labill) or its essential oil, lemongrass leaves or its essential oil (Cymbopogon citratus), mint leaves (Mentha) or its essential oil, lemon (Citrus), ginger (Zingiber officinale), cloves (Syzygium aromaticum), wild honey (Apis mellifera), Tripterygium regelii Sprague & Takeda, Ecklonia cava [65].
Other phytoconstituent can be used: Acacetin, auraptene, cardamonin, daidzein, epicatechin, glabridin, herbacetin, isoxanthohumol and taxifolin hydrate. Adhikari [66] showed antiviral activity by suppressing SARS-CoV 3C protease (3Cpro) [68]. While herbacetin, isobavachalcone, quercetin 3-βD-glucoside, and helichrysetin inhibited MERS-CoV 3Cpro activity [67] while Celastrol, Pristimerin, Tingenone, Iguesterin [69] Dieckol, Eckol, Triphloretol-A, Dioxinodehydroeckol, 2-Phloroeckol, Phloroeckol, PhlorofucofuroeckolA, Fucodiphloroethol G showed activity aginst SARS-CoV [70].
Inhibition of viral spike proteins and receptor: Spike glycoprotein of SARS-CoV-2 contains a receptor-binding domain (RBD) that recognizes the target receptor. The receptorangiotensin-converting enzyme-2 (ACE-2) is a preferable receptor for SARS-CoV-2 [71]. Furin blocks a spike protein of mouse hepatitis coronavirus required for attachment and fusion during infection [73]. Emodin inhibits the spike protein and ACE-2 interaction preventing coronavirus entry [72]. Secondary metabolites like hesperidin, pectolinarin, cannabinoids, rhoifolin, diosmin, apiin, diacetylcurcumin, epigallocatechin gallate, from medicinal plants are bioactive against SARS-CoV-2 main protease and spike glycoproteinso, it is necessary to screen all the available antiviral drugs against COVID-19 for faster development of therapeutic option to control the pandemic [73].
RECENT ONGOING WORK
Medicinal plant are used as potent inhibitors of nucleocapsid phosphoprotein of COVID 19. And for this research phytoleads are used for different computer aided drug desiging, molecular modelling, homology modelling, and different kind of software related SAR studies are ongoing as syntheic molecules. Because phytoleads are also a better choice for treating SARS COV 2 [73].
CONCLUSION
Plants and their phytoleads are much more better option because of great therapeutic value and have minium number of adverse effects as compared to allopathic drugs.Due to this covid 19 pandemic the whole scenerio is shifted to natural products because till now the number of antiviral drugs were used to treat COVID 19 but not a single drug can give promissing result although they reduce the severity of disease and could decrease the rate of mortality. But they also showing some adverse effects. The pharmacological effects of these drugs are also temporary for many of infections. And maximum chances is also their for re-occring of diseases. Phytoleads are always better choice because they are potent and the concept of phytoleads are new because plants having many therapeutic value this is so ancient principle but those phytoleads which are responsible for the partcular illness is a choice of interest. And now all the researchers are going through this. Scientisits are working very much for these phytoleads.
FUTURE PROSPECTIVE
Coming decades are of this natural field. The work of researchers are to investigate these all phytoleads for each and every helth related issue/ ailment. Hopefully in future, all kind of disorders will must be treated by using these phytoleads with potential novel drug delivery system. Computer aided drug desinging will also be very much efficient for these phytolead related discoveries.
CONFLICTS OF INTEREST
The authors declare that they have no conflict of interest.
- Mehta P, Bothiraja C, Mahadik K, Kadam S, Pawar A (2018) Phytoconstituent based dry powder inhalers as biomedicine for the management of pulmonary diseases. Biomed Pharmacother 108: 828-837.
- Laddha AP, Kulkarni YA (2019) VEGF and FGF-2: Promising targets for the treatment of respiratory disorders. Respir Med 156: 33-46.
- Tahergorabi Z, Khazaei M (2012) A review on angiogenesis and its assays. Iran J Basic Med Sci 15(6): 1110.
- Góralczyk B, Drela E, Góralczyk K, Szczypiorska A, Rość D (2012) Angiogenesis in chronic obstructive pulmonary disease. Med Biol Sci 26(3): 19-25.
- Matarese A, Santulli G (2012) Angiogenesis in chronic obstructive pulmonary disease: A translational appraisal. Translat Med 3: 49.
- Voelkel NF, Vandivier RW, Tuder RM (2006) Vascular endothelial growth factor in the lung. Am J Physiol Lung Cell Mol Physiol 290(2): L209-L221.
- To M, Yamamura S, Akashi K, Charron CE, Haruki K, et al. (2012) Defect of adaptation to hypoxia in patients with COPD due to reduction of histone deacetylase 7. Chest 141(5): 1233-1242.
- Walters EH, Soltani A, Reid DW, Ward C (2008) Vascular remodeling in asthma. Curr Opin Allergy Clin Immunol 8(1): 39-43.
- Tuder RM, Yun JH, Bhunia A, Fijalkowska I (2007) Hypoxia and chronic lung disease. J Mol Med 85(12): 1317-1324.
- Fukumura D, Gohongi T, Kadambi A, Izumi Y, Ang J, et al. (2001) Predominant role of endothelial nitric oxide synthase in vascular endothelial growth factor-induced angiogenesis and vascular permeability. Proc Natl Acad Sci U.S.A 98(5): 2604-2609.
- Lee G, Walser TC, Dubinett SM (2009) Chronic inflammation, chronic obstructive pulmonary disease, and lung cancer. Curr Opin Pulm Med 15(4): 303-307.
- Landskron G, De la Fuente M, Thuwajit P, Thuwajit C, Hermoso MA (2014) Chronic inflammation and cytokines in the tumor microenvironment. J Immunol Res 2014: 149185.
- Lee JJ, Natsuizaka M, Ohashi S, Wong GS, Takaoka M, et al. (2010) Hypoxia activates the cyclooxygenase-2-prostaglandin E synthase axis. Carcinogenesis 31(3): 427-434.
- Schuliga M (2015) NF-kappaB signaling in chronic inflammatory airway disease. Biomolecules 5(3): 1266-1283.
- Sangilimuthu A, Sathishkumar R, Priyadarsini DT, Anitha J, Subban R (2015) A review on phytoconstituents against asthma. Int J Pharm Sci Rev Res 30(2): 7-16.
- Zhang H (2011) Anti-IL-1β therapies. Recent Pat. DNA Gene Seq. 5: 126-135.
- Rovina N, Dima E, Gerassimou C, Kollintza A, Gratziou C, et al. (2009) Interleukin-18 in induced sputum: Association with lung function in chronic obstructive pulmonary disease. Respir Med 103(7): 1056-1062.
- Kim HP, Lim H, Kwon YS (2017) Therapeutic potential of medicinal plants and their constituents on lung inflammatory disorders. Biomol Ther 25(2): 91.
- Churg A, Zhou S, Wright JL (2012) Matrix metalloproteinases in COPD. Eur Respir J 39(1): 197-209.
- Chun P (2015) Role of sirtuins in chronic obstructive pulmonary disease. Arch Pharm Res 38(1): 1-10.
- Corhay JL, Henket M, Nguyen D, Duysinx B, Sele J, et al. (2009) Leukotriene B4 contributes to exhaled breath condensate and sputum neutrophil chemotaxis in COPD. Chest 136(4): 1047-1054.
- Hesslinger C, Strub A, Boer R, Ulrich WR, Lehner MD, et al. (2009) Inhibition of inducible nitric oxide synthase in respiratory diseases. Biochem Soc Trans 37(4): 886-891.
- Seimetz M, Parajuli N, Pichl A, Veit F, Kwapiszewska G, et al. (2011) Inducible NOS inhibition reverses tobacco-smoke-induced emphysema and pulmonary hypertension in mice. Cell 147(2): 293-305.
- Marks-Konczalik J, Costa M, Robertson J, McKie E, Yang S, et al. (2015) A post-hoc subgroup analysis of data from a six-month clinical trial comparing the efficacy and safety of losmapimod in moderate-severe COPD patients with ≤ 2% and > 2% blood eosinophils. Respir Med 109(7): 860-869.
- Doukas J, Eide L, Stebbins K, Racanelli-Layton A, Dellamary L, et al. (2009) Aerosolized phosphoinositide 3-kinase γ/δ inhibitor TG100-115 [3-[2, 4-diamino-6-(3-hydroxyphenyl) pteridin-7-yl] phenol] as a therapeutic candidate for asthma and chronic obstructive pulmonary disease. J Pharmacol Exp Ther 328(3): 758-765.
- van der Poll T, Opal SM (2009) Pathogenesis, treatment, and prevention of pneumococcal pneumonia. Lancet 374(9700): 1543-1556.
- File Jr TM (2003) Community-acquired pneumonia. Lancet 362(9400): 1991-2001.
- Mintah SO, Asafo-Agyei T, Archer MA, Junior PA, Boamah D, et al. (2019) Medicinal plants for treatment of prevalent diseases. Pharmacog Med Plant 2019: 1-19.
- World Health Organization (2015) Tuberculosis Fact sheet N 104. 2015. Available online at: http://www.who.int/mediacentre/factsheets/fs104/en
- Van Soolingen D, Hoogenboezem T, De Haas PE, Hermans PW, Koedam MA, et al. (1997) A novel pathogenic taxon of the Mycobacterium tuberculosis complex, Canetti: Characterization of an exceptional isolate from Africa. Int J Syst Evol Microbiol 47(4): 1236-1245.
- Lahm T, Tuder RM, Petrache I (2014) Progress in solving the sex hormone paradox in pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 307(1): L7-L26.
- R.K. Gandharba Ray, Chapter 27 pulmonary arterial hypertension section 4.
- Rabinovitch M (2008) Molecular pathogenesis of pulmonary arterial hypertension. J Clin Invest 118(7): 2372-2379.
- King Jr TE, Pardo A, Selman M (2011) Idiopathic pulmonary fibrosis. Lancet 378(9807): 1949-1961.
- C. Society (2014) Whatisnon-small cell lung cancer? Cancer.Org.
- Frezzetti D, Gallo M, Maiello MR, D’Alessio A, Esposito C, (2017) VEGF as a potential target in lung cancer. Expert Opin Ther Targets 21(10): 959-966.
- Feng P, Zhang ZL, Zhang ZH, Zhang XL, Xiang F, et al. (2013) Effect of endostar combined with cisplatin on expression of VEGF and Sema3A of Lewis lung cancer rats. Asian Pac J Trop Med 6(1): 57-60.
- Singh RP, Gangadharappa HV, Mruthunjaya K (2018) Phytosome complexed with chitosan for gingerol delivery in the treatment of respiratory infection: In vitro and in vivo Eur J Pharm Sci 122: 214-229.
- Chen L, Li J, Luo C, Liu H, Xu W, et al. (2006) Binding interaction of quercetin-3-β-galactoside and its synthetic derivatives with SARS-CoV 3CLpro: Structure-activity relationship studies reveal salient pharmacophore features. Bioorg Med Chem 14(24): 8295-8306.
- Desai A, Desai C, Desai H, Mansuri A, Desai J (2020) Possible Role of Medicinal Plants in COVID-19-a Brief Review. Int J Sci Dev Res 5(4): 205-209.
- Srivastava AK, Chaurasia JP, Khan R, Dhand C, Verma S (2020) Role of medicinal plants of traditional use in recuperating devastating COVID-19 situation. Med Aromat Plants (Los Angeles) 9(359): 2167-2412.
- Wang C, Zheng X, Gai W, Zhao Y, Wang H, et al. (2017) MERS-CoV virus-like particles produced in insect cells induce specific humoral and cellular immunity in rhesus macaques. Oncotarget 8(8): 12686.
- Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, et al. (2020) Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 181(2): 281-292.
- Tortorici MA, Veesler D (2019) Structural insights into coronavirus entry. Adv Virus Res 105: 93-116.
- Rajnik M, Cascella M, Cuomo A, Dulebohn SC, Di Napoli R (2021) Features, Evaluation, and Treatment of Coronavirus (COVID-19). Uniformed Services University of The Health Sciences.
- Rascón-Castelo E, Burgara-Estrella A, Mateu E, Hernández J (2015) Immunological features of the non-structural proteins of porcine reproductive and respiratory syndrome virus. Viruses 7(3): 873-886.
- Turner AJ (2015) ACE2 cell biology, regulation, and physiological functions. The Protective Arm of the Renin Angiotensin System (RAS). 2015:185.
- Jamshidi N, Cohen MM (2017) The clinical efficacy and safety of Tulsi in humans: A systematic review of the literature. Evid Based Complement Alternat Med 2017: 9217567.
- Molla SM, Azad AK, Al Hasib MA, Hossain MM, Ahammed MS, et al. (2019) A Review on Antiviral Effects of Nigella Sativa Pharmacologyonline 2: 47-53.
- Boelaert JR, Piette J, Sperber K (2001) The potential place of chloroquine in the treatment of HIV-1-infected patients. J Clin Virol 20(3): 137-140.
- Keyaerts E, Li S, Vijgen L, Rysman E, Verbeeck J, et al. (2009) Antiviral activity of chloroquine against human coronavirus OC43 infection in newborn mice. Antimicrob Agents Chemother 53(8): 3416-3421.
- Biswas K, Chattopadhyay I, Banerjee RK, Bandyopadhyay U (2002) Biological activities and medicinal properties of neem (Azadirachta indica). Curr Sci 10: 1336-1345.
- Pérez-Jiménez J, Neveu V, Vos F, Scalbert A (2010) Identification of the 100 richest dietary sources of polyphenols: An application of the Phenol-Explorer database. Eur J Clin Nutr 64(3): S112-S120.
- Gülçin İ, Elmastaş M, Aboul-Enein HY (2012) Antioxidant activity of clove oil-A powerful antioxidant source. Arab J Chem 5(4): 489-499.
- Kurokawa M, Hozumi T, Basnet P, Nakano M, Kadota S, et al. (1998) Purification and Characterization of Eugeniin as an Anti-herpesvirus Compound from Geum japonicum and Syzygium aromaticum. J Pharmacol Exp Ther 284(2): 728-735.
- Damle M (2014) Glycyrrhiza glabra (Liquorice)-a potent medicinal herb. Int J Herb Med 2(2): 132-136.
- Cinatl J, Morgenstern B, Bauer G, Chandra P, Rabenau H, et al. (2003) Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus. Lancet 361(9374): 2045-2046.
- Jayakumar T, Hsieh CY, Lee JJ, Sheu JR (2013) Experimental and clinical pharmacology of Andrographis paniculata and its major bioactive phytoconstituent andrographolide Evid Based Complement Alternat Med 2013: 846740.
- Schoeman D, Fielding BC (2019) Coronavirus envelope protein: current knowledge. Virol J 16(1): 1-22.
- Gunathilake KD, Rupasinghe HV (2015) Recent perspectives on the medicinal potential of ginger. Botanics 5: 55-63.
- Wachtel-Galor S, Yuen J, Buswell JA, Benzie IF (2011) Ganoderma lucidum (Lingzhi or Reishi). InHerbal Medicine: Biomolecular and Clinical Aspects. 2nd edn, CRC Press/Taylor & Francis.
- Yu MS, Lee J, Lee JM, Kim Y, Chin YW, et al. (2012) Identification of myricetin and scutellarin as novel chemical inhibitors of the SARS coronavirus helicase, nsP13. Bioorg Med Chem Lett 22(12): 4049-4054.
- Kanyinda JN (2020) Coronavirus (COVID-19): A protocol for prevention and treatment (Covalyse®). Eur J Med Heal Sci 2: 1-4.
- Adhikari B, Marasini BP, Rayamajhee B, Bhattarai BR, Lamichhane G, et al. (2021) Potential roles of medicinal plants for the treatment of viral diseases focusing on COVID‐19: A review. Phytother Res 35(3): 1298-1312.
- Jo S, Kim H, Kim S, Shin DH, Kim MS (2019) Characteristics of flavonoids as potent MERS‐CoV 3C‐like protease inhibitors. Chem Biol Drug Des 94(6): 2023-2030.
- Jo S, Kim S, Shin DH, Kim MS (2020) Inhibition of SARS-CoV 3CL protease by flavonoids. J Enzyme Inhib Med Chem 35(1): 145-151.
- Ryu YB, Park SJ, Kim YM, Lee JY, Seo WD, et al. (2010) SARS-CoV 3CLpro inhibitory effects of quinone-methide triterpenes from Tripterygium regelii. Bioorg Med Chem Lett 20(6): 1873-1876.
- Park JY, Kim JH, Kwon JM, Kwon HJ, Jeong HJ, et al. (2013) Dieckol, a SARS-CoV 3CLpro inhibitor, isolated from the edible brown algae Ecklonia cava. Bioorg Med Chem 21(13):3730.
- Peng C, Zhu Z, Shi Y, Wang X, Mu K, et al. (2020) Yang Y, Zhang X, Xu Z. Exploring the binding mechanism and accessible angle of SARS-CoV-2 spike and ACE2 by molecular dynamics simulation and free energy calculation.
- Ho TY, Wu SL, Chen JC, Li CC, Hsiang CY (2007) Emodin blocks the SARS coronavirus spike protein and angiotensin-converting enzyme 2 interaction. Antivir Res 74(2): 92-101.
- Bosch BJ, Van der Zee R, De Haan CA, Rottier PJ (2003) The coronavirus spike protein is a class I virus fusion protein: Structural and functional characterization of the fusion core complex. J Virol 77(16): 8801-8811.
- Adem S, Eyupoglu V, Sarfraz I, Rasul A, Ali M (2020) Identification of potent COVID-19 main protease (Mpro) inhibitors from natural polyphenols: An in-silico strategy unveils a hope against CORONA.
- Rolta R, Yadav R, Salaria D, Trivedi S, Imran M, et al. (2021) In silico screening of hundred phytocompounds of ten medicinal plants as potential inhibitors of nucleocapsid phosphoprotein of COVID-19: An approach to prevent virus assembly. J Biomol Struct Dyn 39(18): 7017-7034.
-
 Table 1
Table 1 -
Table 2





