Research Article
Association of Heart Inflammation after COVID 19 Vaccination the Systematic Review and Meta-Analysis
2866
Views & Citations1866
Likes & Shares
Introduction: The COVID-19 contamination which developed in December 2019, is caused by the infection SARS-CoV-2. Contamination with this infection can lead to serious respiratory sickness, in any case, myocarditis has too been detailed. The reason of this ponder is to distinguish the clinical highlights of myocarditis in immunized COVID-19 patients.
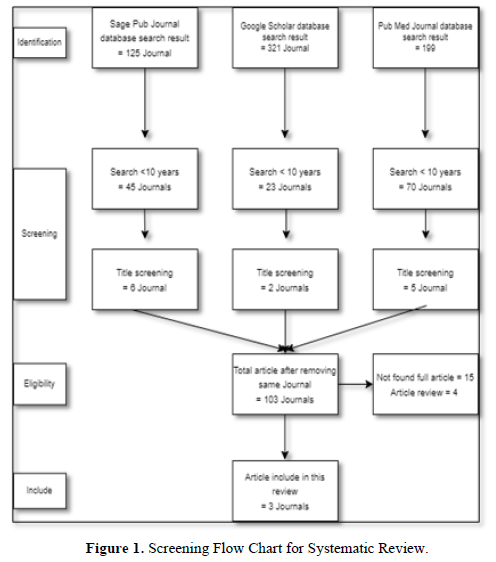
Method: This study using systematic review that search using keyword heart inflammation, myocarditis and Covid-19 Vaccination in Google Scholar, PubMed, and CrossRef. After final screening the author analyze 3 articles.
Result: COVID-19 myocarditis influenced patients over the age of 50 and rates among both sexes were similarly detailed. Patients displayed with dyspnea, hack, fever with hypotension and chest torment. Research facility tests uncovered leukocytosis with expanded C-reactive protein, whereas blood vessel blood gas investigation illustrated respiratory acidosis. All cardiac markers were raised. Radiographic imaging of the chest appeared respective ground glass opacities or reciprocal invades, whereas cardiac attractive reverberation imaging created late gadolinium upgrades. Electrocardiography illustrated ST-segment height or altered T waves, whereas echocardiography uncovered decreased cleared out ventricular launch division with cardiomegaly or expanded divider thickness. Administration with corticosteroids was favored in most cases, taken after by antiviral medicine. The lion’s share of thinks about detailed either recuperation or no encourage clinical disintegration.
Conclusion: Be that as it may, current prove illustrates myocardial aggravation with or without coordinate cardiomyocyte harm, proposing distinctive pathophysiology components mindful of COVID-mediated myocarditis. Built up clinical approaches ought to be sought after until future prove bolster distinctive activities. Huge multicenter registries are prudent to illustrate assist.
Keywords: Heart inflammation, COVID-19 vaccination, Myocarditis
INTRODUCTION
Myocarditis is the dynamic aggravation of the center layer of the heart taken after by a myocardial damage without ischemic occasions [1,2]. The irresistible and non-infectious causes of myocarditis decide its prognostic results. The (focal/diffuse) degrees of myocardial aggravation decide the seriousness of side effects in patients with myocarditis [1]. The age/gender-appropriate burden of myocarditis was recorded as 6.1/100,000 for men and 4.4/100,000 for ladies (inside the age extend of 35-39 a long time) in 2019 [3]; be that as it may, myocarditis-related mortality affected 0.2/100,000 men and 0.1/100,000 ladies within the same year. The clinical thinks about uncover the most noticeably awful results with ineffectively caught on obsessive pathways in 20-30% of hospitalized COVID-19 (coronavirus malady) patients with myocardial harm [4].
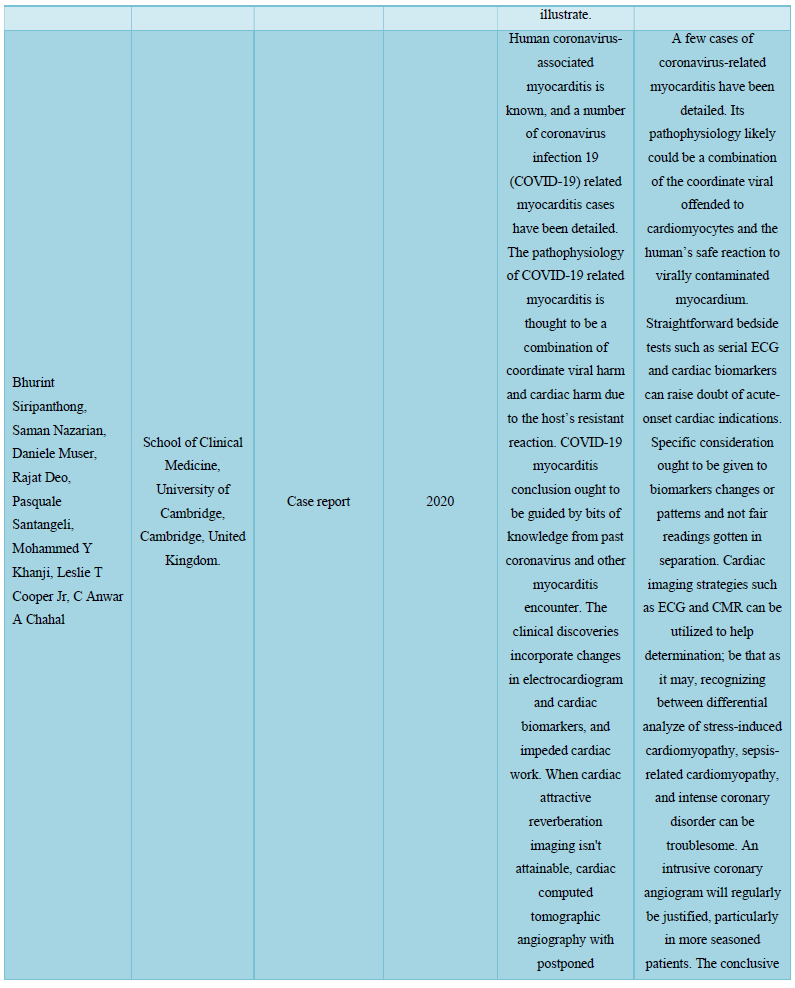
Myocarditis, a fiery condition influencing the myocardium, comes about from a wide range of both irresistible and non-infectious causes. Numerous diverse infections have been embroiled, counting the Center East Respiratory Disorder (MERS) coronavirus [5], which closely takes after SARS-CoV-2. Myocarditis is suspected on the premise of lifted troponins within the patient’s blood, cardiac arrythmias or diffuse ST height on electrocardiogram (ECG) and cleared out ventricular divider movement variations from the norm (territorial or worldwide hypokinesis) on echocardiogram. The clinical introductions of myocarditis incorporate subclinical, subacute, intense and fulminant shapes, and abrupt-onset myocarditis is known to be related with critical seriousness [6].
METHODS
This study using systematic review that search using keyword heart inflammation, myocarditis and Covid-19 vaccination in Google Scholar, PubMed, and CrossRef. After final screening the author analyze 5 articles. As in methods, the author summarizes 3 articles that mention in Figure 1.
DISCUSSION
Viral myocarditis continuously breaks down the center layer of the heart through myocardial damage activated by incendiary forms [2]. The viral etiology of myocarditis is predominantly detailed within the Joined together States and other created countries of the world [1]. Viral myocarditis advances with virus-mediated cardiomyocyte harm driven by improper enactment of natural and versatile resistant frameworks. The intense, subacute, and incessant stages of viral myocarditis respond with the degree of cardiomyocyte disintegration and versatile safe reactions.
The intense stage of myocarditis advances with the intrusion of infection particles into the cardiomyocytes, taken after by their cleavage, repackaging, and connection to MHC (major histocompatibility complex)-1 receptors on the cell film. This occasion is taken after by the official of CD8+ (cytotoxic) T-cells to the class-I MHC particles on virus-infected cardiomyocytes, subsequently actuating apoptosis and ensuing discharge of cardiac and viral antigens (Figure 1) [6]. The authoritative of viral antigen to toll-like receptors (TLRs) on antigen-presenting cells (APCs) actuates NF-kB translation figure that potentiates the qualities included within the biosynthesis and discharge of pro-inflammatory cytokines (TNF-α, IFN-γ, IL-1, IL-6, and IL-12), subsequently activating the adaptive safe reactions within the subacute stage. The virus-mediated cytotoxicity eventually actuates cardiomyocyte apoptosis and early myonecrosis within the tainted quiet [7].
The versatile safe reactions overwhelm the virus-mediated cardiomyocyte harm through cellular penetration of lymphocytes amid the subacute stage. The early stages of the subacute stage advance with the dynamic repackaging of viral antigens within the antigen-presenting cells (APCs) and their interaction with MCH-II receptors. The intense stage shows with the connection of antigen-bound MHC II receptors (on APCs) with the CD4+ Aide T cells that triggers numerous versatile safe reactions interceded by proinflammatory cytokines [7].
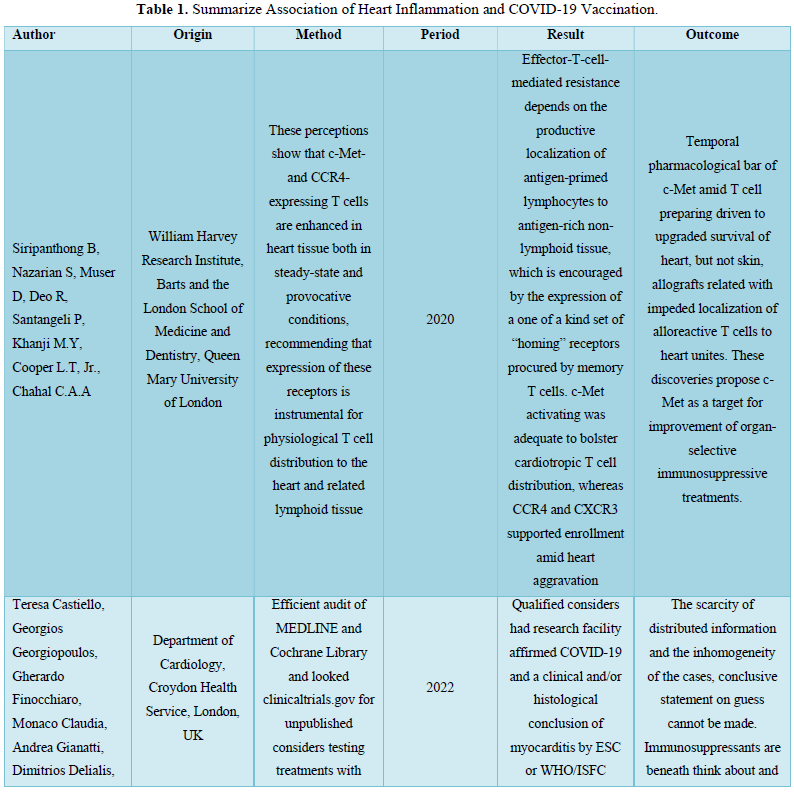
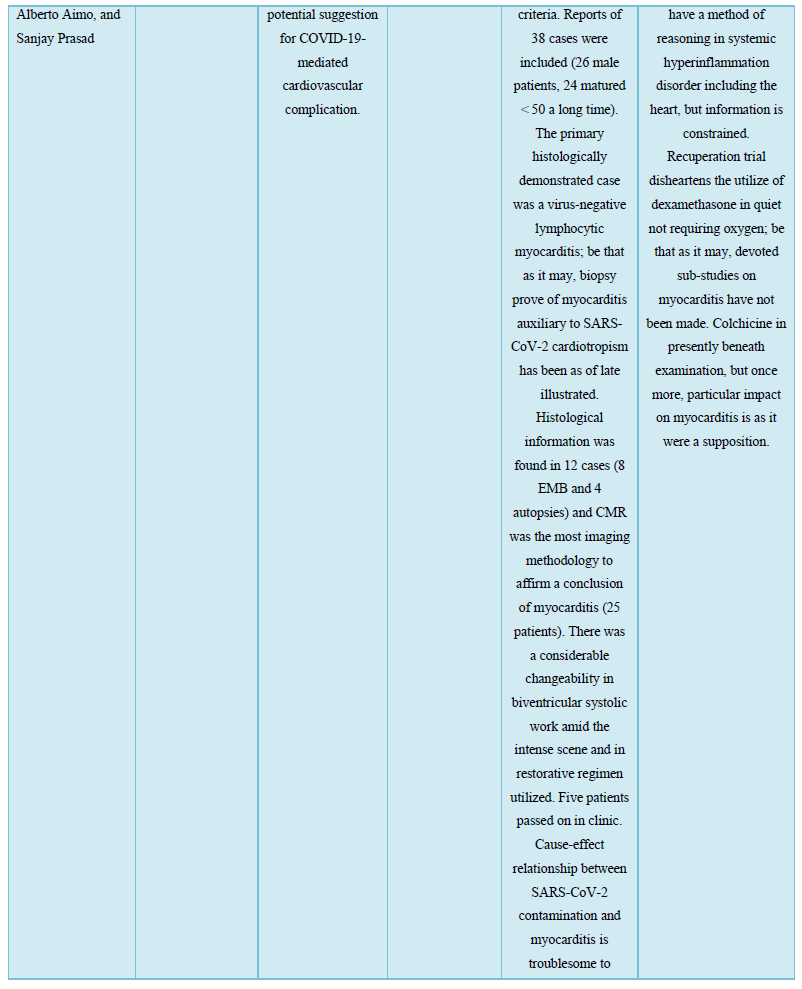
The hoisted cytokines (IFN-γ and IL-12) initiate Th1 separation and advance assist enactment of macrophages and cytotoxic T cell-mediated harm [8]; in any case, IL-12 height potentiates the movement of common executioner (NK) cells. The actuated Th cells tie to the antigen-oriented MHC II receptors on B-cells to advance the arrangement of virus-specific antibodies and autoreactive antibodies against the cardiac antigens and myosin [9]. The late subacute stage shows with the sequestration of viral antigen-oriented actuated dendritic cells by lymph hubs and preparing of naïve T-cells against SARS-CoV-2 tainted cells [10]. The unremitting stage of viral myocarditis (Table 1).
Advances with Myocardial Fibrosis, Heart Disappointment, and Widened Cardiomyopathy
The actuated spike (S) proteins of SARS-CoV-2 particles associated with angiotensin-converting enzyme-2 (ACE2) on the target cells to intervene their section into the have framework. The ACE2 receptor expression happens in cardiomyocytes after the interruption of SARS-CoV-2 into the epithelial cells lining the respiratory tract and sort II pneumocytes [12]. The cardiomyocyte harm by SARS-CoV-2 may take after abnormal safe reactions that create in other sorts of viral myocarditis. Future clinical considers still require depicting the pathophysiological forms administering myocardial harm and myocarditis in patients with COVID-19.
The coordinate cell damage and T-lymphocyte cytotoxicity increased by IL-6 intervened cytokine storm (CS) administer the pathophysiology of viral myocarditis [7]. The checked rise within the proinflammatory cytokines counting, IL-6, IL-8, and TNF-α in seriously sick SARS-CoV-2 patients recommends that CS improvement may play a vital part within the clinical movement of COVID-19 [13,14]. The movement of monoclonal-antibody (like tocilizumab) against the IL-6 receptors in COVID-19 pneumonia patients includes to their therapeutic administration within the current situation [15,16].
The clinical thinks about to emphasize the part of the HGF-c-MET (transmembrane tyrosine kinase) pivot within the pathogenesis of SARS-CoV-2 initiated myocardial harm [17]. The localized irritation inside the heart advances with cardiomyocyte discharge of hepatocyte development figure (HGF) and its interaction with the c-MET receptors on naïve T cells in lymph hubs [17,18]. The natural myocardial forms and immune-mediated hyperinflammatory reactions taking after viral presentation moreover decide the pathophysiological components of SARS-CoV-2 myocarditis [19].
Administration of Myocarditis due to COVID-19 Contamination or Immunization
The symptomatology of COVID-19 infection-induced or post-vaccine-related myocarditis incorporates shortness of breath, weariness, and chest torment. Patients with tall seriousness myocarditis regularly report the signs of right-sided heart disappointment, counting lifted jugular venous weight, right upper quadrant torment, and fringe edema [20]. Few patients with COVID-19 moreover create extreme diffuse cardiac aggravation driving to fulminant myocarditis, ventricular arrhythmias, and cardiogenic stun. Fulminant myocarditis as a rule creates inside 2-3 weeks of contracting the infection and presents with ventricular brokenness and intense onset of heart disappointment [18]. CDC advocates myocarditis screening for patients who create shortness of breath, chest torment, or palpitations inside 7 days of getting the mRNA COVID-19 immunization [21]. The more youthful patients with COVID-19 indications moreover require myocarditis screening to run the show out their coronary attribution.
Administration of COVID-19 contamination or antibody related myocarditis
The current treatment methodologies supposedly don't demonstrate advantageous for patients with COVID-19 infection or vaccine-related myocarditis. The current therapeutic administration of COVID-19-related myocarditis depends on corticosteroids and intravenous immunoglobulins (IVIG) to challenge the movement of diffuse non-specific resistant framework enactment [18,27]. The adequacy and security of corticosteroids in COVID-19 scenarios, in any case, warrant encourage examination. The evidence-based myocarditis administration rules by AHA and ESC confine the utilization of nonsteroidal anti-inflammatory drugs (NSAIDs) based on their attribution for renal impedance and sodium maintenance which will worsen intense ventricular/LV systolic brokenness in COVID-19 related myocarditis patients [1,18,23]. The COVID-19 patients may assist require heart disappointment treatment based on their hemodynamic soundness and cardiac yield [19].
The demonstrative examination ought to run the show out fulminant myocarditis in COVID-19 patients with sepsis some time recently regulating intravenous liquid revival to play down the hazard of lethal complications. Besides, cardiogenic stun in fulminant myocarditis regularly goes with ventricular tachyarrhythmias and bradyarrhythmia overwhelmed by a heart square, syncope, and sudden cardiac passing [20]. The current AHA rules advocate the usage of cardiogenic stun administration treatment convention for patients with fulminant myocarditis. The mechanical circulatory bolster by extracorporeal layer oxygenation (ECMO), a ventricular help gadget (VAD), or an intra-aortic swell pump may help the long-term restorative administration of hemodynamically unsteady COVID-19 patients with myocarditis [18].
COVID-19 immunization actuated myocarditis
The clinical information for most patients with myocarditis did not uncover their showing side effects (barring eight patients with chest torment as their displaying complaint) [28-30]. The clinical discoveries encourage affirmed myalgia in two patients and fever in one case [28,29]. The information advance clarified the onset of myocarditis in patients after a few weeks of getting the COVID-19 antibody [31]. The patients detailed myocarditis side effects inside three days of accepting the first/second measurements; be that as it may, most introductions related with the moment measurements of the COVID-19 antibody. The understanding we examined created myocarditis indications inside two days of accepting the COVID-19 immunization. The therapeutic writing uncovered COVID-19 vaccine-related myocarditis patients inside the age gather of 20-30 a long time, not at all like our understanding, who had completed her 6th decade of life.
The persistent we examined displayed with T-wave reversals that coordinated the ECG discoveries recorded for three cases within the therapeutic writing. We assist taken note T-wave reversals in two patients and ST-segment height in twelve of the detailed seventeen cases [28-31]. The ECG discoveries assist related with the cardiac biomarker heights and serum troponin peaks at changing levels within the enrolled patients. The discoveries from our quiet at first uncovered a typical troponin level that along these lines trended upwards amid her therapeutic management. The seventeen cases we recovered from the restorative writing displayed with a protected discharge division, barring one persistent who created apical hypokinesia [28].
The persistent we overseen displayed a essentially diminished launch division (10%) and cleared out ventricular dyskinesia. She had a restricted pretest likelihood for ACS within the nonattendance of cardiac hazard variables. The persistent declined cardiac catheterization in spite of the therapeutic suggestion. We advance taken note cardiac catheterization attempted for thirteen out of seventeen patients enlisted within the therapeutic writing [28-31]. The patients who gotten cardiac catheterization had no history of coronary course illness. The raised cardiac markers and chest pain demonstrated to be the most noteworthy confounders within the symptomatic appraisal of myocarditis. We managed obtrusive mechanical ventilation and vasopressor bolster to our understanding unguided by a cardiac MRI. The seventeen cases detailed in therapeutic writing, in any case, gotten cardiac MRI during their restorative administration. Our discoveries advance uncovered a stamped height within the procalcitonin level (185 ng/mL) of the myocarditis persistent.
CONCLUSION
The results of this case situation affirm myocarditis as a plausible complication of COVID-19 antibodies. The differential evaluation of patients with COVID-19 immunization status and side effects of intense cardiac decompensation must run the show out myocarditis to maintain a strategic distance from deadly complications. An early conclusion is key to play down COVID-19 vaccine-related misfortunes and make strides the therapeutic administration of patients suspected of myocarditis. In addition, the author will continue to support halal treatment based on the Quran and Sunnah in the intervention against Covid-19 which is much safer and is blessed by Allah SWT and Rasulullah Muhammad.
ACKNOWLEDGMENT
The author would like to say alhamdulillah, sholawat and hopefully continue to be devoted to the great prophet Muhammad and his family. The author would also like to thank Maryam and Isa Clinic and beloved mom and dad for their support so far.
- Santoso A, Pranata R, Wibowo A, Al-Farabi MJ, Huang I, et al. (2020) Cardiac injury is associated with mortality and critically ill pneumonia in COVID-19: A meta-analysis. Am J Emerg Med 44: 352-357.
- Tian W, Jiang W, Yao J, Nicholson CJ, Li RH, et al. (2020) Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J Med Virol 92(10): 1875-1883.
- Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, et al. (2020) Synthesis without meta-analysis SWiM in systematic reviews: Reporting guideline. BMJ 368: l6890.
- Ogilvie D, Fayter D, Petticrew M, Sowden A, Thomas S, et al. (2008) The harvest plot: A method for synthesizing evidence about the differential effects of interventions. BMC Med Res Methodol 8: 8.
- Cooper LT Jr, Keren A, Sliwa K, Matsumori A, Mensah GA (2014) The global burden of myocarditis: part 1: A systematic literature review for the Global Burden of Diseases Injuries and Risk Factors 2010 study. Glob Heart 9: 121-129.
- Shi S, Qin M, Shen B, Cai Y, Liu T, et al. (2020) Association of Cardiac Injury with Mortality in Hospitalized Patients With COVID-19 in Wuhan. JAMA Cardiol 5(7): 802-810.
- Guo T, Fan Y, Chen M, Wu X, Zhang L, et al. (2019) Cardiovascular implications of fatal outcomes of patients with coronavirus disease COVID-19. JAMA Cardiol 5(7): 811-818.
- Bonow RO, Fonarow GC, OGara PT, Yancy CW (2020) Association of coronavirus disease 2019 COVID-19 with myocardial injury and mortality. JAMA Cardiol 5(7): 751-753.
- Zheng YY, Ma YT, Zhang JY, Xie X (2020) COVID-19 and the cardiovascular system. Nat Rev Cardiol 17: 259-260.
- Ruan Q, Yang K, Wang W, Jiang L, Song J (2020) Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan. China Intensive Care Med 46: 846-848.
- Peretto G, Sala S, Caforio ALP (2020) Acute myocardial injury MINOCA or myocarditis Improving characterization of coronavirus-associated myocardial involvement. Eur Heart J 41: 2124-2125.
- Oudit GY, Kassiri Z, Jiang C, Liu PP, Poutanen SM, et al. (2009) SARS coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur J Clin Invest 39: 618-625.
- Escher F, Pietsch H, Aleshcheva G, Bock T, Baumeier C, et al. (2020) Detection of viral SARS CoV2 genomes and histopathological changes in endomyocardial biopsies. ESC Heart Fail 7: 2440-2447.
- Wan S, Yi Q, Fan S, Lv J, Zhang X, et al. (2020) Characteristics of lymphocyte subsets and cytokines in peripheral blood of 123 hospitalized patients with 2019 novel coronavirus pneumonia NCP. Available online at: https://www.medrxiv.org/content/10.1101/2020.02.10.20021832v1.full.pdf
- Liu T, Zhang J, Yang Y, Zhang L, Ma H, et al. (2020) The potential role of IL-6 in monitoring coronavirus disease 2019. Available online at: https://www.medrxiv.org/content/10.1101/2020.03.01.20029769v2.full.pdf
- Gong J, Dong H, Xia S, Huang Y, Wang D, et al. (2020) Correlation analysis between disease severity and inflammation related parameters in patients with COVID-19 pneumonia. Available online at: https://www.medrxiv.org/content/10.1101/2020.02.25.20025643v1.full.pdf
- Basso C, Aguilera B, Banner J, Cohle S, d Amati G, et al. (2017) Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows Arch 471: 691-705.
- Caforio AL, Pankuweit S, Arbustini E, Basso C, Gimeno-Blanes J, et al. (2013) Current state of knowledge on etiology diagnosis management and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 34: 2636-48
- Zhou F, Yu T, Du R, Fan G, Liu Y, et al. (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan China: A retrospective cohort study. Lancet 395: 1054-1062.
- Calabrese LH (2020) Cytokine storm and the prospects for immunotherapy with COVID-19. Cleve Clin J Med 87(7): 389-393.
- Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, et al. (2020) COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 395: 1033-1034.
- Friedrich MG, Sechtem U, Schulz-Menger J, Holmvang G, Alakija P, et al. (2009) Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol 53: 1475-1487.
- Baughman KL (2006) Diagnosis of myocarditis death of Dallas criteria. Circulation 113: 593-595.
- Bracamonte-Baran W, Čiháková D (2017) Cardiac autoimmunity myocarditis. Adv Exp Med Biol 1003: 187-221.
- Fujioka M, Suzuki K, Iwashita Y, Imanaka-Yoshida K, Ito M, et al. (2019) Influenza associated septic shock accompanied by septic cardiomyopathy that developed in summer and mimicked fulminant myocarditis. Acute Med Surg 6: 192-196.
- Basso C, Leone O, Rizzo S, De Gaspari M, van der Wal AC, et al. (2020) Pathological features of COVID-19 associated myocardial injury: A multicenter cardiovascular pathology study. Eur Heart J 41: 3827-3835.
- Wenzel P, Kopp S, Göbel S, Jansen T, Geyer M, et al. (2020) Evidence of SARS CoV2 mRNA in endomyocardial biopsies of patients with clinically suspected myocarditis tested negative for COVID-19 in nasopharyngeal swab. Cardiovasc Res 116: 1661-1663.
- Wichmann D, Sperhake JP, Lütgehetmann M, Steurer S, Edler C, et al. (2020) Autopsy findings and venous thromboembolism in patients with COVID-19: A prospective cohort study. Ann Intern Med 173: 268-277.
- Xiong TY, Redwood S, Prendergast B, Chen M (2020) Coronaviruses and the cardiovascular system acute and long-term implications. Eur Heart J 41: 1798-1800.
- Merken J, Hazebroek M, Van Paassen P, Verdonschot J, Van Empel V, et al. (2018) Immunosuppressive therapy improves both short- and long-term prognosis in patients with virus-negative nonfulminant inflammatory cardiomyopathy. Circ Heart Fail 11: e004228.
- Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L, et al. (2021) Dexamethasone in hospitalized patients with Covid-19 preliminary report. N Engl J Med 384(8): 693-704.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4







