Journal of Psychiatry and Psychology Research (ISSN:2640-6136)

Review Article
The Effect of Psychological Intervention on Self Esteem and Depression on children with HIV
4105
Views & Citations3105
Likes & Shares
The present study aimed to find the effect of the psychological intervention on the Self-Esteem and Depression of children who have been infected with Human Immuno deficiency Virus (HIV). The psychological intervention comprised of a combination of life skills training program coupled with counseling for a period of three months. Beck’s Depression inventory and Rosenberg’s Self-Esteem questionnaires were used to measure the dependent variables. Due to the nature of the population studied, ex-post facto research design was adopted and purposive sampling was used. The difference between Pre-test and Posttest of the intervention was measured using the t-test. It was found that the psychological intervention had helped in reducing the depression and enhanced the self-esteem of the children affected by HIV. Findings of the study were discussed in the light of the results obtained.
Keywords: Life skill training, Depression, Self-esteem, HIV
INTRODUCTION
AIDS may be a condition during which progressive failure of the system allows life-threatening opportunistic infections and cancers to thrive which is caused by HIV. Without treatment, average survival time after infection with HIV is estimated to be 9 to 11 year. HIV is majorly a sexually transmitted infection. However non-sexual transmission can occur from an infected mother to her infant during pregnancy, during childbirth by exposure to her blood or vaginal fluid, and thru breast milk. It also can be transmitted through unscreened transfusion and contaminated needle usage. HIV by itself isn't a killer disease. It paves way for the opportunistic infectious diseases causing life threatening symptoms which makes living a challenge. It makes it difficult for the adults to stick to medicines and sustain life. All the more the co morbid conditions like cancer and other diseases make it difficult to adapt to medicine dependent life. Within the cases of youngsters infected by HIV, the insight about the illness and awareness about the consequences of treatment is extremely low because it makes medical adherence a challenging task to them. The number of youngsters becoming newly infected with HIV remains unacceptably high. In 2016, around 160,000 children became infected with HIV. The bulk of youngsters living with HIV are infected via mother-to-child transmission, during pregnancy, childbirth or breastfeeding.
Most of the youngsters after their disclosure of HIV status become orphans. Within the cases of orphans and vulnerable children, the devastating impact of HIV is that the loss of whole generations of individuals in communities by the epidemic. HIV treatments for youngsters’ work. Thanks to limited range of age-appropriate antiretroviral (ART) drugs, it makes treatment difficult as ART is that the life sustaining aid.
Many children living with HIV experience tough life events that would affect their psychosocial wellbeing, like losing caregivers to AIDS-related illnesses, stigma, shock about their status, and not understanding the importance of adhering to treatment. Studies are conducted to review the varied factors like stigma, income of the family, care giver bias that have an impression on the psychological state of youngsters suffering from HIV. [1]. These factors create high risk in resulting in psychological state problems like poor quality of life, lack of social support and medical adherence.
As far as interventions are concerned for this population only a really few areas are researched upon. Cognitive behavioral characteristics derived from the Information-Motivation-Behavioral Skills model of health promotion behaviors showed that ladies who had missed a minimum of one dose of their HIV medications within the past week reported lower intentions motivation to stay adherent. Although medical adherence, be the first aid, the psychological Intervention also plays a serious role in domains like hope in life, self-esteem, depression thanks to physical ailments, thoughts about death and resilience. Meta-analysis of cognitive-behavioral interventions on HIV-positive person’s psychological state and immune functioning. CBIs are efficacious in improving various psychological states [2].
From the prevailing literature, it had been found that depression is prevalent among individuals suffering from HIV between 4.9%-17.9 % with major symptoms of depression. [3] Therefore, this study aims at studying the amount of depression. Depressive symptoms were significant predictors of low self-esteem among the individuals with HIV were acknowledged by [4]. Supported this structural link within the literature psychological intervention was incorporated. The intervention included life skills training (LST) and counseling. Life skills training have been used extensively among children. LST was found to reinforce Self-esteem among school students [5]. Life skills training as intervention was found to extend social and emotional development and social adjustment. With regards to counseling individuals with HIV, its emphasis was on the medical adherence, stigma and risky sexual behaviors. Counseling has been found to be very useful to the adults in bringing holistic. Since there was a scarcity of studies using life skills training among children with HIV, the present study incorporated life skills training including counseling as a psychological intervention program to reinforce their overall psychological state wellbeing. Life skills provide an overall readiness to face social challenges and can power to beat certain physical ailments [6]. Life skills also teach individuals to spice up their confidence and help them build a positive outlook on life. This exploratory research may be a pioneering attempt within the field of psychological state in India.
PROBLEM STATEMENTS
Does psychological intervention have an impact on Depression and Self-Esteem among children with HIV? (Table 1).
OBJECTIVES
To study the relationship between Self-Esteem and Depression of the children infected with HIV.
To find out the effect of psychological intervention on the Self-Esteem and Depression of the children infected with HIV.
Hypothesis
Depression and Self-Esteem of children with HIV will be not related. (H1)
Psychological intervention will have no effect on the Depression among children with HIV. (H2)
Psychological intervention will have no effect on the Self-Esteem among children with HIV. (H3)
Method of investigation
The study aimed to find the effect of independent variable- psychological intervention on the dependent variables Depression and Self-Esteem of children with HIV [7]. The sample comprised of sixteen girls and fourteen boys (30) from the age range 10-18 years. The nature of study was ex-post facto and purposive sampling technique was used to select the participants.
Tools used
Beck’s depression questionnaire by [8] which is a self-scoring inventory was used to measure the depression of children with HIV. The internal consistency ranges from 0.73 to 0.92.
Rosenberg’s self-esteem questionnaire was used to evaluate the self-esteem of the participants. [9] It was devised by [10]. It has an internal consistency of 0.77 and test retest reliability of 0.90. Along with which a personal data sheet was used to collect other demographic information such as socioeconomic status and age.
Before and after without control design was used. The t-test to find the effect of the intervention based on the pre-test and post-test measures of the dependent variables.
Main Study
The main study was conducted in four phases as follows: Formulation of the psychological intervention, Pre-test assessment, Implementation of the training program and Post-test assessment.
PHASE 1
Formulation of the intervention
The psychological intervention comprised of life skills training and individual counseling. It aimed to enhance the Self-Esteem and decrease the depressive symptoms of the children with HIV. Therefore, the intervention program focused on three areas such as Interpersonal skills, Academic skills and personal competencies for 18 days spread over six months.
- Interpersonal skills- Communication, Bullying and assertiveness, Peer involvement, importance of family and relationship, dealing with Stigma, Concept of love, marriage.
- Personal competencies- Self Esteem and confidence building, Emotions, self-awareness, anger management, resilience, Suicidal ideas and coping strategies, motivation, time management, responsibility.
- Academic skills- Importance of education, study skills, memory techniques.
- Counseling sessions were based on an eclectic approach. Group counseling was done for 5 session and individual counseling sessions were carried out based on the intensity of the problem and child’s needs.
PHASE 2
Pre-test assessment
The participants were elaborated with need and significance of the study and motivated to participate actively. Confidentiality was ensured to the participants and they were encouraged to be honest in answering the questionnaires [11]. Depression and Self-Esteem levels were assessed using chosen questionnaires. A personal data sheet was used to collect other demographic details.
PHASE 3
Implementation of the Psychological intervention
The intervention was spread over six months. Initial three months were utilized to conduct life skills training program and the latter three months were used to carryout individual counseling.
The Life skills training program used activities, role plays, games, and debate and group discussions to elucidate the concepts to the children. Each session lasted for about 4 hr a day for 18 days that was spread across three months during the weekends.
PHASE 4
Post-test assessment
The post-test evaluation was conducted after the intervention was completed.
STATISTICAL ANALYSIS
Pearson’s correlation method was used to assess the relationship between the [12]. Depression and Self-Esteem of the children with HIV. The paired‘t’-test was used to examine the difference between pre-test and post-test scores.
RESULTS AND DISCUSSION
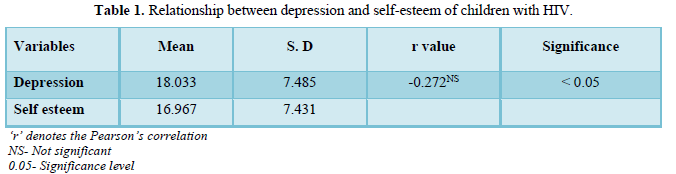
In Table 1, it is learnt that the correlation between Depression and Self-Esteem r = - 0.272 is not significant. This means that there is no relationship between self-esteem and depression of the children with HIV. Therefore hypotheses (H1) “Depression and Self-Esteem will be not related” is accepted.
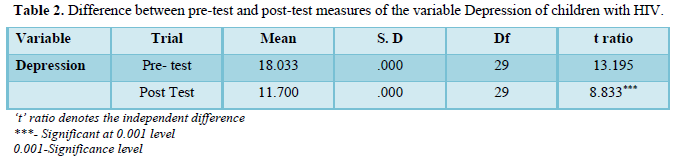
In Table 2, it is learnt that the ‘t’ ratio is 8.833 and is significant at 0.01 level. The mean differences between Pre-test and Post-test scores of depression, it indicates that there is a significant decrease in the post test scores of depression. Therefore, the null hypothesis (H2) ‘Psychological intervention will have no effect on depression’ is rejected.
This could be due to majority of the children were orphans. It is not surprising as majority of the sample chosen were orphans subjected to a very low caretaker-child ratio (1:8). Thus, through the intervention program the children got an opportunity to share their problems and would have been benefited by counseling sessions which eventually helped in reducing the levels of depression.
Independent “t” ratio between Pre-test and Post-Test measures of Depression among children with HIV
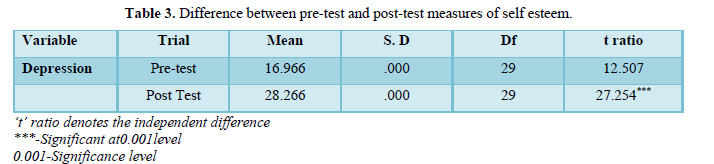
In the below Table 3 it is learnt that the t-ratio 27.254 is found to be significant at 0.001 level. This means that the Psychological intervention had significantly increased the level of self-esteem. Therefore hypotheses (H3) ‘Psychological intervention will have no effect on Self-Esteem’ was rejected.
This shows that the psychological intervention was advantageous to the sample and is in line with the existing literature on self-esteem. As the psychological intervention included life skills and counseling, life skills would have helped in enhancing self-esteem as its methodology was experiential in nature.
Independent “t” ratio between Pre-test and Post- Test measures of Self-Esteem among children with HIV
IMPLICATIONS OF THE STUDY
The present research was confined to the study of only self-esteem and depression among children with HIV due to constraint of time. However, though the study was restricted to thirty sample size (n=30), its findings are of both theoretical and practical significance with numerous implications [13,14]. The findings of the present study could be of practical utilization when training programs are designed in future to foster the mental health among the children with HIV this strengthens the theoretical knowledge pertaining to the related variables. It also highlights the need for the role of counselors in institutions providing care for children with HIV.
CONCLUSION
The findings of the study clearly bring out the efficacy of Psychological intervention in reducing the depression and enhancing the self-esteem of children affected by HIV. Thus, psychological intervention including life skills training and counseling serves as a powerful strategy in dealing with children with HIV. Hence all the mental health professionals and care givers dealing with children and individuals affected by HIV can confidently use this intervention.
- Freeman M, Thom R (2006) Serious mental illness and HIV / AIDS. S Afr J Psychol 12(1): 4-8.
- Crepaz N, Passin WF, Herbst JH, Rama SM, Malow RM, et al. (2008) Meta-analysis of cognitive-behavioral interventions on HIV-positive persons mental health and immune functioning. Health Psychol 27(1): 4-14.
- Olatunji BO, Williams BJ, Haslam N, Abramowitz JS, Tolin DF (2008) The latent structure of obsessive-compulsive symptoms: A taxometric study. Depress Anxiety 25(11): 956-968.
- Ramam S (2014) A study on the assessment of symptoms and severity of major depression among individuals with HIV/AIDS - A report from South India. Int J Pharm Edu Res 1(2): 81-85.
- Bierman KL, Furman W (1984) The effects of social skills training and peer involvement on the social adjustment of preadolescents. Child Dev 55(1): 151-162.
- Botvin GJ & Griffin KW (2014) Life skills training: Preventing substance misuse by enhancing individual and social competence. New Directions for Youth Development 2014(141): 57-65.
- Grinstead OA, Gregorich SE, Choi KH, Coates T (2001) Positive and negative life events after counseling and testing: The Voluntary HIV-1 Counseling and Testing Efficacy Study. AIDS 15(8): 1045-1052.
- Beck AT, Ward CH, Mendelson M., Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4: 561-571.
- Navarro RT (2014) Self-esteem Influences Depressive Symptoms among Female Sex Workers. IAMURE Int J SocSci 10(1).
- Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press.
- Ndebele M, Hara MK, Greyling M (2012) Application of the information, motivation and behavioural skills model for targeting HIV risk behaviour amongst adolescent learners in South Africa. SAHARA-J: J Soc Aspects HIV/AIDS 9(sup1): S37-S47.
- Okanda M (2017) Do social pressures facilitate children’s yes bias? The Proceedings of the Annual Convention of the Japanese Psychological Association 81: 2C-077.
- Sublette NK (2008) Predictors of depressive and anxiety symptoms among african american hiv-positive women. University of Tennessee Health Science Center.
- Tuthill EL, Butler LM, Pellowski JA, Mcgrath JM, Cusson RM, et al. (2017) Exclusive breast-feeding promotion among HIV-infected women in South Africa: An Information–Motivation–Behavioural Skills model-based pilot intervention. Public Health Nutr 20(8): 1481-1490.



QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Chemotherapy Research Journal (ISSN:2642-0236)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Rheumatology Research (ISSN:2641-6999)


