Journal of Oral Health and Dentistry (ISSN: 2638-499X)

Review Article
Acceptance to a “Sugar Free Campus” Concept in a Dental College: A Questionnaire Based Study
5887
Views & Citations4887
Likes & Shares
Introduction: Sugar is a risk factor for dental caries, obesity and various health conditions. Promoting a healthy food environment enables people to adopt and maintain healthy dietary practices. Hence, a precise and comprehensive assessment is required to assess the willingness of a dental institute towards sugar restrictions in the campus.
Aim: To assess the acceptance to a “sugar free campus” concept in a dental college: a questionnaire-based study.
Methodology: A validated 14-point questionnaire-based study tool was administered to the staff, postgraduates and undergraduates of the college in this cross-sectional study. The assessment was done using a 5-point Likert scale for each question. The questionnaire also included a section for additional comments.
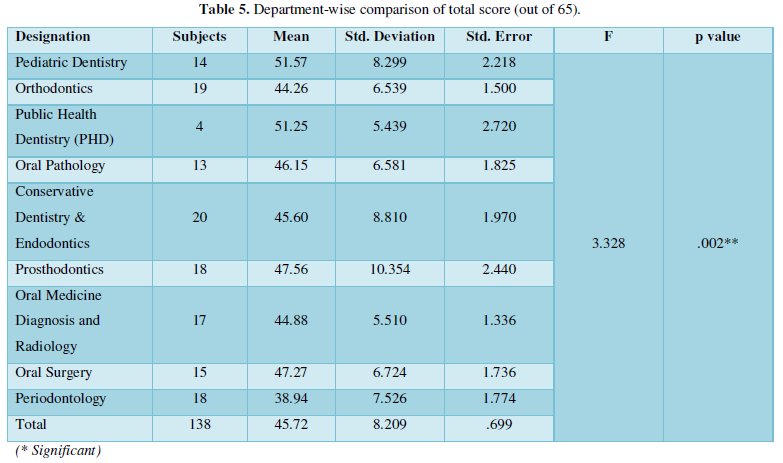
Results: 451 eligible questionnaires were obtained (response rate: 90%). Mean score of 45.37 ± SD 7.567 was obtained across the study population (N = 451). Highest score was seen in lecturers (mean 49.39 ± 8.176) and lowest score was seen in 1st year postgraduates (mean 41.79 ± 7.544). Highest score was seen in Pediatric Dentistry department (mean 51.57 ± 8.299), lowest was seen in Periodontology department (mean 38.94 ± 7.526). The most strongly agreed upon concept was availability of sugar free tea/coffee as an option in CDE programmes. The most strongly disagreed upon concept was restriction on celebrating birthdays in the institute premises.
Conclusion: There was a mixed acceptance to a “sugar free campus” concept with variations across departments and designations.
Keywords: Free sugars, Dental caries, Tobacco free campus, Upstream approach, Prevention, Health promotion
Abbreviations: WHO: World Health Organization; CDE: Continuing Dental Education; BDS: Bachelor of Dental Surgery; PHD: Public Health Dentistry; SSB: Sugar Sweetened Beverages; NCDs: Non-communicable diseases
INTRODUCTION
Marmot [1] had mentioned that ‘people's lifestyles and the conditions in which they live and work strongly influence their health and longevity’. Dietary behavior is governed by the accessibility, availability, affordability and acceptability of choosing healthy food options over unhealthy ones [2]. Subsequent to the WHO sugar guidelines (2015) [3], the objective of reduction in sugar consumption necessitates an upstream approach [4]. Changing work environment has been proven as an effective strategy in curbing tobacco use initiation, second hand smoke exposure, and the social acceptability of tobacco use [5]. Several studies have observed significant reduction in smoking prevalence among university students by adoption of ‘Tobacco free campus’ concept [6,7]. Similar strategy for sugar control could be a revolutionary idea. A dental school is an ideal environment for developing a model workplace for restriction of sugar consumption as dentists often advise sugar control.
However, no study regarding acceptability of a ‘sugar free campus’ in dental schools has been reported. Therefore, a study was undertaken to assess the willingness of a dental institute towards sugar restrictions in the campus.
AIM
The study aimed at assessing the acceptance to a “sugar free campus” concept in a dental institute.
OBJECTIVES
- To assess the acceptance of the “sugar free campus” concept based on the overall score obtained
- To assess the designation-wise acceptance to the “sugar free campus” concept
- To assess the department-wise acceptance to the “sugar free campus” concept
- To compare the differences in the acceptance to the “sugar free campus” concept w. r. t. the gender, designations and departments.
MATERIALS AND METHODS
A questionnaire-based cross-sectional study design was used for this study. Necessary clearances were obtained from the Institutional Review Board and Institutional Ethics Committee, prior to beginning of the study. Required permission was taken from the dean and a written consent was obtained from each participant. The study was conducted in a private dental institute in an urban area (Dr. G. D. Pol’s Foundation Y.M.T. Dental College and Hospital, Kharghar, Navi Mumbai). The sample comprised of approximately 80 dental staff members, 95 postgraduates and 400 undergraduates including the interns. The first-year undergraduates were excluded as their term had not started. The study was conducted during the period: 2nd August to 10thAugust, 2018.
Study tool
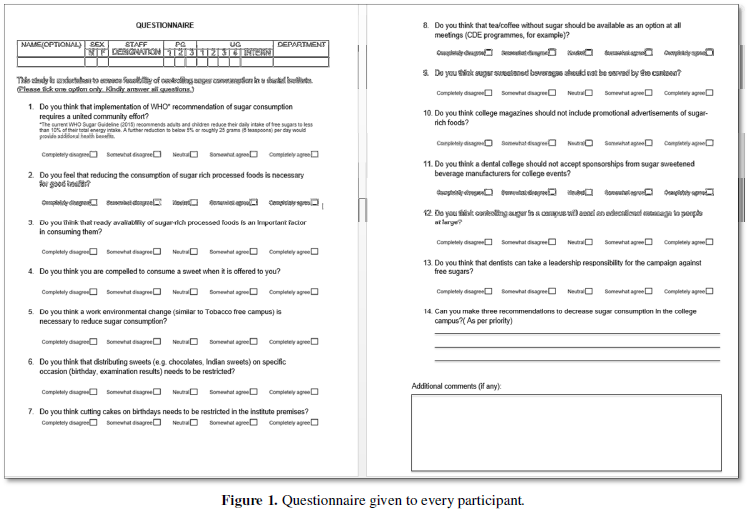
This being a novel study, a study tool comprising of 14-point questionnaire (Figure 1) was developed. The questionnaire was piloted in a different school and also validated by an expert. Since the dental curriculum in this institution follows the English language, information sheet, consent form and questionnaire were provided in the English language only. The tools were physically distributed to about 500 participants in the entire college. A personal reminder was given after 5 days to participants who had not filled the questionnaire. We managed to collect 451 questionnaires at the end of the study.
Data sources/ measurement
The assessment was done using a 5-point Likert scale ranging from completely disagree (scored as 1) to completely agree (scored as 5). The level of acceptance was measured in terms of total score out of the maximum (65) as a quantitative continuous variable. The questionnaire also included one open ended question “Can you make three recommendations to decrease sugar consumption in the college campus? (Write in the order of preference)” to judge the attitude of the participants qualitatively. The questionnaire also included a section for additional comments which was optional. The modifying factors considered in the study were gender, designation and department to which the participant belonged.
RESULTS
Data obtained were compiled on a MS Office Excel Sheet (2013) and subjected to statistical analysis using Statistical Package for Social Sciences (SPSS v 21.0, IBM). Data were not normally distributed and non-parametric tests were used. For all the statistical tests, significance level of 0.05 was chosen (p<0.05).
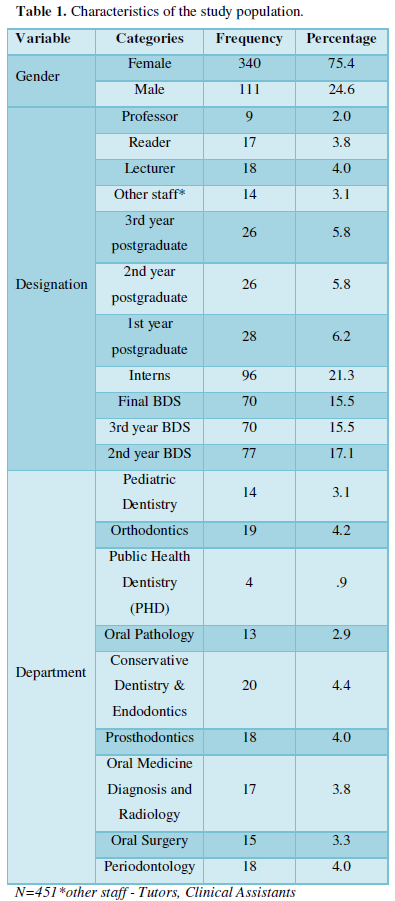
The characteristics of the study population in terms of their gender, designation and department are shown in Table 1. Out of the entire study population, seventy five percent were females. There were eleven designations and nine departments. The distribution is shown both in frequencies and percentages.
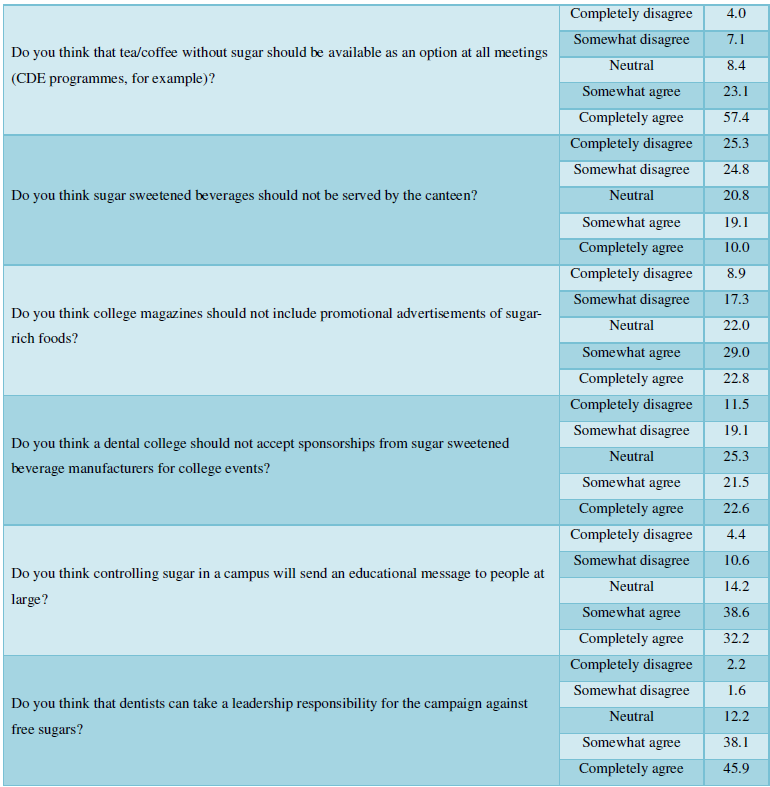
451 eligible questionnaires were obtained (response rate= 90%). The minimum possible score was 13 and maximum possible score was 65. Mean score of 45.37 (± 7.567) was obtained in the study population (N = 451). Table 2 depicts the overall percentage of various responses to all questions. 80% of the study population agreed that a reduction in consumption of sugar rich processed foods is necessary for good health. 80% of the study population also agreed to availability of sugar free tea/coffee options at conferences etc., in the college campus. 63% and 53% of the study population disagreed on restriction on cake cutting for birthdays and distribution of sweets on special occasions, respectively.
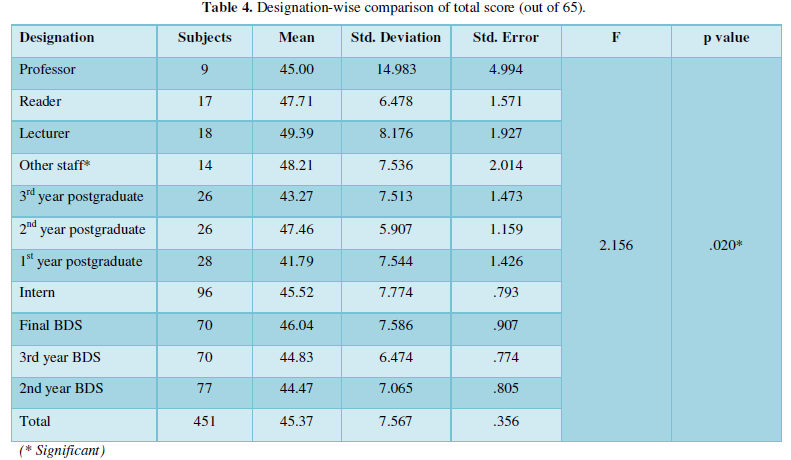
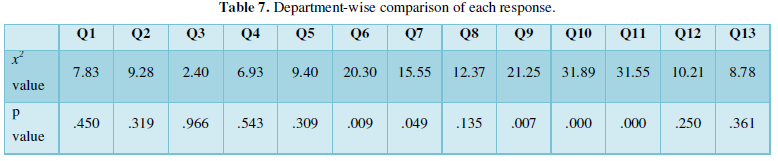
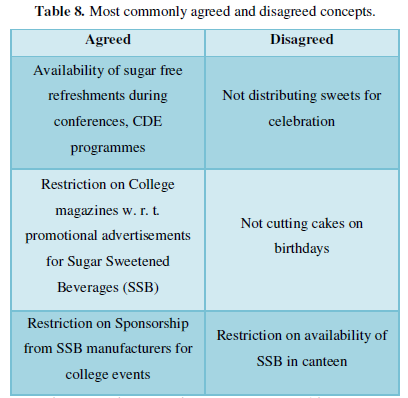
Comparison of the mean score (out of 65) was done with respect to gender, designation and department using the t-test and f-test. Statistically non-significant difference was seen w. r. t. the gender but significant differences were seen for different designations and departments (Tables 3-7). Highest score was seen with lecturers and lowest was seen with 1st year postgraduates. There was a higher acceptability of this concept with respect to Pediatric Dentistry and Public Health Dentistry departments as compared to the Periodontology and Orthodontics departments. Designation-wise and department-wise, both, we found statistically significant differences in the responses to certain set of questions. Based on the various responses we could summarize the most commonly agreed and disagreed concepts as stated in Table 8.



Overall, there was a significant difference between the responses given by staff, postgraduate and undergraduate students. A greater acceptance of the concept was shown by the staff when compared to postgraduate and undergraduate students.
With regards to open ended questions, we came across interesting concepts which were noteworthy. The participants suggested putting up educational posters and conducting educational seminars in the campus regarding the ill-effects of free sugar; celebrating birthdays on a common day and following a “no sugar day” in the campus.
DISCUSSION
As many as 3.5 billion people are affected by oral diseases globally [8]. Untreated dental caries is the most prevalent health condition globally affecting all age groups and is governed by its chronic progressive and cumulative pattern causing pain, discomfort, economic burden and negative impact on oral health quality of life. [9,10]. Obesity similar to dental caries is largely preventable but has now become a serious health concern of the 21st century. Free sugar consumption, tobacco use, and harmful alcohol consumption, as well as the wider social and commercial determinants of health are the common risk factors of oral conditions and other non-communicable diseases (NCDs) [11].
Over the past 50 years, worldwide sugar consumption has tripled and is expected to grow [12]. Several corporate, social and cultural practices have led to a belief that sugar is a source of harmless pleasure [12,13]. However, enough evidence already exists that free sugar, similar to tobacco, is toxic and contributes to the global burden of NCDs [14]. Amplifying global advocacy on reduction of free sugar consumption is now a mainstream health priority [15]. Dentists advocate healthy dietary practices to their patients. However, in addition to such simple, individualistic and educational approaches, an upstream health promotional approach is the need of the hour.
A dental college can be an ideal model for health behavior change w. r. t. sugar reduction. It is important to understand the attitude of dental staff and students towards free sugar consumption as these individuals are the oral health ambassadors. Since dentists can take a leadership responsibility in a campaign against free sugars, we conducted this research - one of its kinds, in a dental campus to assess the acceptance to “sugar free campus” using a questionnaire.
In our study, we found that staff and students were aware of the ill effects of sugar but that did not translate into readiness for a “sugar free campus”. This could possibly be because the human brain adores the “status quo” [16]. Changing behavior is extremely difficult and having people accepted to radical change is complex [17]. However, we could find a changing trend in some departments. The higher acceptance of Pediatric Dentistry and Public Health Dentistry departments towards this concept could be because these specializations focus more on prevention and health promotion compared to Periodontology, Conservative Dentistry and Endodontics departments, which indulge more in treatment interventions. Overall, greater acceptance to the concept was seen by the teaching staff as compared to postgraduate and undergraduate students. We found that amongst different designations, lecturers had the highest acceptance to the concept which could be attributed to their increased involvement in conducting dental camps (educational), greater interaction with the patients and conducting lectures for undergraduates. The fresh batches of postgraduates and undergraduates had the least acceptance probably because they may lack the understanding of the implications of free sugars on health.
Food industry, through its various marketing strategies, sponsorships of various conferences, etc., has a profound influence on people’s food choices, purchases and consumption patterns [18]. Restriction on sponsorships for college events and advertisements in college magazine could be necessary. By adopting a “sugar free campus” concept, dental schools can influence their patients and visitors to adopt and maintain healthy dietary practices. It is stated that “physicians who practice healthy lifestyle norms are more likely to convince and benefit their patients to follow the same” [19]. Dentists can thus ‘lead by example’ for the reduction of sugar consumption.
OUR STUDY HAS FOLLOWING LIMITATIONS
This being a preliminary investigation a convenient sample from only one institute was chosen. The group sizes were not equal (undergraduates were more in number as compared to staff and postgraduates; and professors were much fewer than lecturers as is seen in any teaching institute). Moreover, the teaching practices, campus restrictions, social and cultural practices, food availability, etc. vary from place to place and thus, this study has limited generalizability. However, this being the first study of its kind, has made important observations and generated important hypotheses to be tested.
CONCLUSIONS
There was a mixed acceptance to a “sugar free campus” concept. Significant variations to the concept were seen w. r. t. designations and departments but not w. r. t. gender. Pediatric Dentistry and Public Health Dentistry showed highest acceptance whereas Department of Periodontology showed the least acceptance towards the “sugar free campus” concept. Teaching staff showed higher acceptance compared to students.
A multicentric study with a larger sample can substantiate the claims made by our study. Furthermore, studies assessing the knowledge and behaviors of staff and students of dental schools in addition to the attitude towards the “sugar free campus” concept are necessary. A stepwise implementation of “sugar free campus” will bring in an environmental change that is much necessary for the prevention of NCDs and dental conditions.
DISCLAIMER
The authors declare no conflict of interest. This study was self-funded.
- World Health Organization (2003) Wilkinson RG, Marmot M, editors. Social determinants of health: the solid facts. Available online at: https://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf
- National Research Council (2013) Supplemental nutrition assistance program: Examining the evidence to define benefit adequacy. National Academies Press.
- World Health Organization (2015) Guideline: Sugars intake for adults and children. Geneva. Available online at: https://www.who.int/publications/i/item/9789241549028
- World Cancer Research Fund International. Curbing global sugar consumption. Effective food policy actions to help promote healthy diets & tackle obesity. Available online at: https://www.wcrf.org/wp-content/uploads/2021/01/Curbing-Global-Sugar-Consumption.pdf
- Wang TW, Tynan MA, Hallett C, Walpert L, Hopkins M, et al. (2018) Smoke-free and tobacco-free policies in colleges and universities - United States and territories, 2017. MMWR Morb Mortal Wkly Rep 67(24): 686 -689.
- Seo D-C, Macy JT, Torabi MR, Middlestadt SE (2011) The effect of a smoke-free campus policy on college students' smoking behaviors and attitudes. Prev Med 53(4-5): 347-352.
- Lechner WV, Meier E, Miller MB, Wiener JL, Fils-Aime Y (2012) Changes in smoking prevalence, attitudes, and beliefs over 4 years following a campus-wide anti-tobacco intervention. J Am Coll Health 60(7): 505-511.
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators (2018) Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159): 1789-1858.
- Bernabé E, Sheiham A (2014) Age, period and cohort trends in caries of permanent teeth in four developed countries. Am J Public Health 104(7): e115-e121.
- Sheiham A (2006) Dental caries affects body weight, growth and quality of life in pre-school children. Br Dent J 201(10): 625-626.
- World Health Organization (WHO). Global health Observatory (GHO) data: Noncommunicable diseases (NCD). Available online at: https://www.who.int/data/gho/data/themes/noncommunicable-diseases
- World Dental Federation (2015) The challenge of oral disease: A call for global action. The oral health atlas. 2nd Geneva: FDI.
- Kickbusch I, Allen L, Franz C (2016) The commercial determinants of health. Lancet Glob Health 4(12): e895-e896.
- Kharbanda OP, Moynihan P, Priya H, Ivaturi A, Gupta A, et al. (2018) Report from a symposium on accelerating policy-driven action against excessive sugar consumption for the prevention of early childhood caries and noncommunicable diseases. Indian J Public Health 62(4): 305.
- Watt RG, Daly B, Allison P, Macpherson LM, Venturelli R, et al. (2019) Ending the neglect of global oral health: time for radical action. Lancet 394(10194): 261-272.
- Samuelson W, Zeckhauser R (1988) Status quo bias in decision making. J Risk Uncertain 1(1): 7-59.
- Kelly MP, Barker M (2016) Why is changing health-related behavior so difficult? Public Health 136: 109-116.
- Hastings G, McDermott L, Angus K, Stead M, Thomson S (2006) The extent, nature and effects of food promotion to children: A review of the evidence. Geneva. World Health Organization.
- Klein D, Guenther C, Ross S (2016) Do as I say, not as I do: Lifestyles and counseling practices of physician faculty at the University of Alberta. Can Fam Physician 62(7): e393-e399.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
-
Table 9










QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Rheumatology Research (ISSN:2641-6999)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)



