Journal of Oral Health and Dentistry (ISSN: 2638-499X)

Case Report
Management of Immature Mandibular Premolar Tooth with Periapical Lesion Using Single Step Biodentine Apexification - A Case Report
4186
Views & Citations3186
Likes & Shares
The primary goal of endodontic treatment of a tooth is to eliminate all microorganisms from the root canal and provide hermetic seal of the canal space which prevents recurrence of infection. The immature teeth associated with any periapical abnormalities or pulpal infection poses an extreme endodontic treatment difficulty due to absence of apical stop for obturating material. But the treatment trend of providing apical closure using apical barrier has gained popularity known as apexification procedure. The present case report describes the successful management of the mandibular premolar tooth associated with periapical pathology using single step apexification with the help of biodentine.
Keywords: Single step apexification, Biodentine, Immature mandibular premolar
Abbreviation: MTA: Mineral trioxide aggregate
INTRODUCTION
In the eruption stage of permanent teeth, the completion of root development and closure of root apex takes approximately 3 years. During this stage of root development any trauma to the teeth, caries causing pulpal necrosis leads to inflammation of periradicular tissues, interruption of root development associated with periapical pathology [1]. The non-vital tooth with open apex poses a great challenge to the Endodontists. Previously the available treatment options are filling the canal with paste fills or apical surgery. Nowadays, the available treatment options are apexification and regenerative endodontics. Regenerative endodontics has more advantages than apexification in terms of establishing natural structures instead of providing artificial apical matrix [2,3]. But the main disadvantages of the regenerative endodontics are when associated periapical pathology is large, the inducing bleeding from the canal is difficult. So, the treatment option is apexification in case of immature teeth associated with large periapical lesion. Apexification is defined as the treatment option of inducing calcified barrier in the tooth with open apex by the formation of mineralized hard tissue in the apical region of the tooth with necrotic pulp [4]. Apexification procedure includes single step and multiple step apexification procedures. Various materials are used for apexification which includes 1. Calcium hydroxide - previously used materials have two main drawbacks. They are time consuming that it will take 4 or 5 months to form initial calcified barrier and calcium hydroxide used in canal for longer time causes less fracture resistance of dentin 2. MTA - the gold standard material foe apexification procedure. However longer is the time for setting, discoloration of tooth, difficult handling properties, and the biodentine has become popular for treating immature tooth to overcome the negative properties of MTA [5,6]. So, the present case report uses biodentine for apexification procedure for treating the immature central incisor associated with periapical pathology.
CASE REPORT
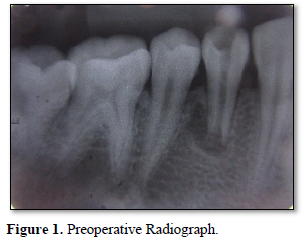
A 20-year-old young female patient presented with a chief complaint of pain in the lower right back tooth region for past 1 month. Previous history revealed that he had a trauma at his 9 years of age. His medical history was non-contributory. Intraoral examination revealed discoloration of crown and grade 1 mobility, with already access opening was attempted by general dentist and referred to our department for specialty treatment in relation to 45. The tooth showed tender to percussion. Tooth mobility and probing depth was within their normal physiologic limit. Thermal and electric pulp test elicits negative response in 45. Radiographic examination revealed fracture of enamel and dentin associated with periapical lesion around the immature root apex of 45. Based on clinical and radiographic analysis, provisional diagnosis was made as pulp necrosis with symptomatic apical periodontitis and apexification treatment was decided.
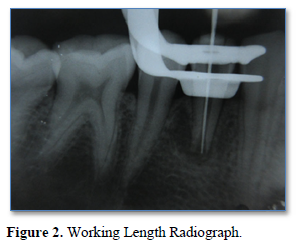
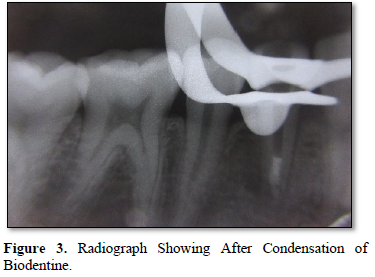
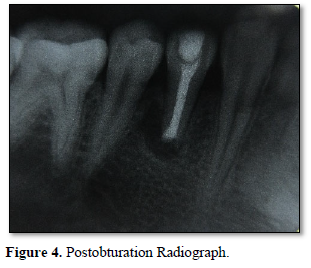
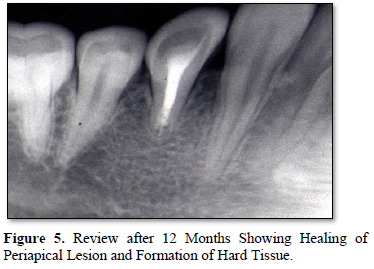
After administering local anesthesia, rubber isolation was made. The access cavity was prepared with the help of Endo access and Endo Z bur. After creating straight line access, the working length was measured with the help of conventional radiograph by using 80 no k file. After confirming the working length, cleaning and shaping of the cavity was done by 80 no k file in a circumferential manner. The canal was irrigated with 2.5 % NAOCL and final irrigation was done with normal saline. Then calcium hydroxide medicament dressing was done. After 2 weeks patient was recalled and cavity is irrigated with NAOCL and normal saline. The canals were dried with paper points. After drying the canal Biodentine was mixed according to the manufacturer’s instructions and condensed into the canal carefully with the help of plugger until it creates 5 mm of apical plug. The remaining canal space is obturated with gutta-percha. Finally, the cavity is restored with composite restoration (Figures 1-5).
DISCUSSION
The endodontic treatment for tooth with immature apex comprises of Apexogenesis, Apexification and Regenerative endodontics. Apexogenesis is the formation of complete root only when the vital pulp tissue presents in the pulp canal. Regenerative endodontics provides healing rate of about 90 to 100 %, but in apexification procedures the success rate is 93.5 for single visit apexification and 90.5 % for two visit apexification [7]. The advantage of regenerative endodontic procedure is formation of pulp- dentin complex and providing natural host defense to the tooth. However few drawbacks have been considered, as it necessitates long term follow up for results. Apexification may be carried by multiple visit or single visit procedure. Calcium hydroxide is the traditionally used material for multiple visit apexifications. Even though Calcium hydroxide apexification is easier and more reliable technique, but poses many drawbacks which include longer treatment time, bacterial contamination in between appointments, inconvenience to patients as it comprises of more follow up visits, increased chance of tooth fracture due to loss of fracture resistance of dentin [8]. To overcome the drawbacks of multiple visit procedure, newly introduced calcium silicate cements provide better option in apexification procedure. The gold standard material for apexification is MTA. Apart from numerous advantages, because of its longer setting time, discoloration property with grey MTA, difficult handling properties, a new tricalcium cement Biodentine was introduced with superior properties to overcome the disadvantages of MTA. The constituents are tricalcium silicate, calcium carbonate and zirconium oxide. The liquid contains calcium chloride in a water-soluble polymer [9]. It is considered as the alternative to MTA in many aspects such as setting time of 12 min whereas for MTA 2 h 45 min. Then comparatively Biodentine showed least micro leakage when it is used as root end filling material [10]. It is also called as dentin substitutes because of its superior handling properties, elastic modulus, compressive strength, micro hardness as comparable with normal dentin. So, when used as apical plug of 5mm provides excellent seal which prevents micro leakage and also provides antibacterial action which results in long term success of apexification. Study conducted by Han and Okiji, revealed that the Ca and Si rich layers over root dentin was found higher in Biodentine when compared to MTA [11]. Biodentine induces pulpal cell proliferation leads to differentiation of odontoblast like cells results in mineralization [12]. Also produces better dentinal bridge under osteodentin and stimulates fibroblast formation. Because of these superior qualities, Biodentine plays a most important material of choice in the single step apexification procedures.
CONCLUSION
For many years Calcium hydroxide is widely used for apexification in case of necrotic teeth with immature open apex. Recent trend changed from multiple visit calcium hydroxide apexifications to single step MTA apexification procedure. However due to minor drawbacks of MTA, a new biocompatible material Biodentine was introduced to overcome the disadvantages of MTA. The superior properties of Biodentine results in better healing and higher success rate in apexification. However long-term follow-up and clinical investigations are further required.
- Bhasker SN (1991) Orban’s Oral Histology and Embryology. 11th St. Louis: Mosby-Year Book; pp: 382.
- Navin M, Isha N, Neelam M (2013) Platelet-rich fibrin-mediated revitalization of immature necrotic tooth. Contemp Clin Dent 4(3): 412-415.
- American Association of Endodontists (2013) Glossary of Endodontic Terms. Accessed on: November 06, 2013. Available online at: http://www.aae.org/
- Balasubrahmaniam A, Sabna BS, Kumar MR, Jayasree S (2014) one visit apexification using a novel dental material, Biodentine - A case report. IOSR J Dent Med Sci 13(5): 90-92.
- Jose J, Shoba K, Faizal CP, Tomy N, Aman S (2015) One step apexification with two bioactive materials - A CBCT evaluation. Int J Oral Health Med Res 2: 46-49.
- Isha N, Neelam M, Navin M (2015) A comparative evaluation of the blood clot, platelet-rich plasma and platelet - rich fibrin in regeneration of necrotic immature permanent teeth: A clinical study. Contemp Clin Dent 6(1): 63-68.
- Witherspoon DE, Small JC, Regan JD, Nunn M (2008) Retrospective analysis of open apex teeth obturated with mineral trioxide aggregate. J Endod 34: 1171-1176.
- Maroto M, Barbería E, Planells P, Vera V (2003) Treatment of a non‑vital immature incisor with mineral trioxide aggregate (MTA). Dent Traumatol 19: 165-169.
- Laurent P, Camps J, DeMéo M, Déjou J, About I (2008) Induction of specific cell responses to a Ca (3) SiO (5) ‑ based posterior restorative material. Dent Mater 24: 1486-1494.
- Leiendecker AP, Qi YP, Sawyer AN, Niu LN, Agee KA, et al. (2012) Effects of calcium silicate-based materials on collagen matrix integrity of mineralized dentin. J Endod 38: 829-833.
- Han L, Okiji T (2011) Uptake of calcium and silicon released from calcium silicate‑based endodontic materials in to root canal dentine. Int Endod J 44: 1081-1087.
- Zanini M, Sautier JM, Berdal A, Simon S (2012) Biodentine induces immortalized murine pulp cell differentiation in to odontoblast-like cells and stimulates bio mineralization. J Endod 38: 1220-1226.





QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Pathology and Toxicology Research
- Journal of Rheumatology Research (ISSN:2641-6999)
- BioMed Research Journal (ISSN:2578-8892)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)



