Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)

Research Article
Radiological Predictors of Depressed Calvarial Fractures Associated Injuries
4672
Views & Citations3672
Likes & Shares
Purpose: To discuss different varieties of injuries associated with depressed skull fractures at the site of injury and the possibility of predicting them preoperatively.
Methods: Preoperative radiology scans and intra-operative findings for patients who underwent surgery for depressed skull fractures for the year 2020 in a tertiary university emergency hospital were analyzed. Non-contrast CT of the head was the standard examination in cases of head trauma, MRI and MRV were indicated only when dural venous sinus injury was suspected.
Results: 46 patients were included in the study, 36 of them were males. Twelve patients showed dural tear intra-operatively. The dural tear was associated with an average angulation of 27 degrees compared to 18 degrees for patients with intact dura. Depression depth in the dural tear group was 1.8 cm (range =0.5-5 cm) and 1.26 cm for the intact dura group (range =0.5-2.5 cm). Pneumocephalus was found in 18 patients (at the site of injury (6/12), remote and parenchymal (5/18), only parenchymal (1/18). All patients with remote and/or parenchymal pneumocephalus showed a dural tear.
Conclusion: Depressed fractures associated injuries are predictable pre-operatively in most of cases, which is essential to prospect for adequate surgical theater, blood transfusion and neurosurgical expertise preparation.
Keywords: Depressed fracture, Dural tear, Cerebral contusion, Head trauma
INTRODUCTION
Depressed skull fracture is one of the common sequelae of head trauma with an incidence of 16 % among head trauma patients, because of the solid skull structure, a trauma strong enough to cause a depressed segment is usually sufficient to cause brain damage [1]. Depressed fracture associated injuries are those which are caused by the direct head blow, or due to the sharp edge of the bone fragments [2]. Surgical management of depressed fractures is most likely to be indicated to avoid the late sequelae such as infection and seizures [3]. Though depressed fractures are not solely life-threatening condition, associated injuries like epidural hematoma, Dural tear, cerebral contusion, cerebral laceration and Dural sinus injury can be serious and fatal [4]. CT has become the imaging modality of choice for diagnosis of cranial traumatic injury because of its availability, speed, and cost-effectiveness. Predicting associated injuries is essential to plan surgical procedure properly based on data obtained from the standard imaging technique. In this article we are putting in focus injuries that are associated with depressed skull fractures at site and time of trauma, rather than injuries resulted from same head impact irrelevant to the depressed fracture and how to predict such injuries using CT scan.
METHODS
Patient Selection
This retrospective study was approved by the local institutional review board and a waiver of the consent of medical record review was received. Medical records of the surgical theater of a tertiary university emergency hospital were reviewed for the year 2020, patients who underwent surgery for depressed skull fractures were identified and their medical records were examined. Patients who were managed conservatively were not included, as the radiological signs were confirmed according to intra-operative findings from operative details registry.
CT technique and analysis
Non-enhanced CT (NECT) was performed with a 160-slice CT machine (Aquilion Prime 160 Slice), image analysis was conducted on the PACS system (GE Healthcare, Waukesha WI).
Pneumocephalus in our study was classified into three categories; (i) extra-axial at site of injury which can be subdural or epidural as they couldn’t be differentiated radiologically, (ii) remote extra-axial pneumocephalus which is mostly intradural, and (iii) parenchymal pneumocephalus which is certainly intradural.
Angulation of the depression is defined in this study as the highest angle between the depressed segment and an imaginary curve connecting the two adjacent non-depressed edges, while depth of depression was calculated as the distance between the deepest point of the depressed segment and the imaginary curve. Relation of fracture to Dural venous sinus and distance in between were reported. (Figures 1A & 1B)
Magnetic Resonance Venography (MRV) was indicated only for patients with depressed fractures directly overlying one of the dural venous sinuses. The scans were performed on a 1.5 Tesla MRI scanner (Philips, Netherland).
Intra-operative findings
Intra-operative findings included Dural tear, sinus laceration which required repair and sinus bleeding which was categorized as a different entity which required no sinus repair. These findings were considered apart from the surely diagnosed pathologies on preoperative CT scans, like EDH and cerebral contusion.
RESULTS
The study included 46 patients, 36 of them were male. Age ranged from 1 to 60 years old with mean age of 19.13 years. Thirty-six patients were fully conscious at time of presentation (GCS 15) while 4 patients’ score was 14, four patients with moderate head trauma and two with severe head trauma. (Table 1).
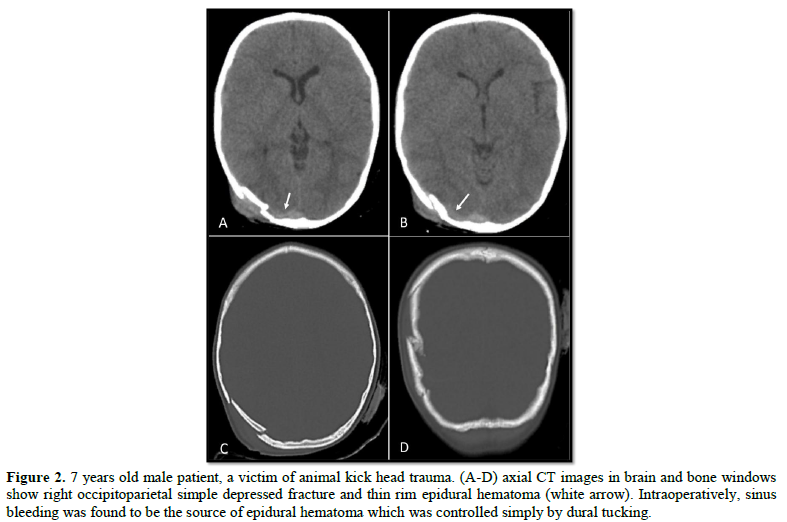
Contusion was found in 10/46 representing 21.7 %, dural tear was associated with contusion in (6/10) 60 % cases. Epidural hematoma was associated with depressed fracture in 10/46 (21.7%). (Figures 2-6) are demonstrative cases.
Intraoperatively, there was a dural tear, there was no dural sinus bleeding nor injury.
The diameter of the depressed segment ranged from 1.5 to 6 cm with a mean diameter of 3.98 cm. Angulation of the depressed segment ranged from 0˚ (no angulation) in 18 patients to 85°, with a mean angulation of 20.65°. Depression depth ranged from 0.5 cm to 5 cm with mean of 1.4 cm. 12 patients showed Dural tears intraoperatively, for this group, the mean angulation and depth were 27 degrees and 1.8 cm respectively, compared to 18 degrees and 1.26 for the intact dura group (Table 2).
Mann Whitney test was performed to confirm or exclude correlation of depth and angulation to dural tear. Although depth of the depressed segment was higher in the dural tear group, it was not statistically significant. On contrary, increased angulation of the depressed segment was strongly correlated to Dural tear (P= 0.01). Pneumocephalus was a CT finding in 18 patients, 5 of them showed remote and parenchymal pneumocephalus while one patient showed only parenchymal pneumocephalus. The other 12 showed pneumocephalus at site of injury only. All patients with remote and/or parenchymal pneumocephalus showed Dural tear intraoperatively. Dural tear was found in all patients with remote and/or parenchymal pneumocephalus (6/6) and two with local extra-axial pneumocephalus (2/12). Four patients of the Dural tear group showed no pneumocephalus on preoperative CT scans. Twenty fractures were related to Dural venous sinus, 8 of them were directly over the sinus while the other 12 were close to the sinus with 1-2 cm distance range. The most related sinus was superior sagittal sinus (SSS) with an incidence of 14/20, followed by transverse sinus (TS) for four patients and both for two patients. One patient of the 8 (12.5 %) sinus overlying fractures was associated with attenuation of flow in superior sagittal sinus and transverse sinuses due to depressed segment compression in MRV. Sinus laceration that required repair was found in 50% of the fractures overlying a dural venous sinus (4/8), while sinus bleeding in epidural space was encountered in eight patients of the depressed fractures in the sinus vicinity (8/12).

DISCUSSION
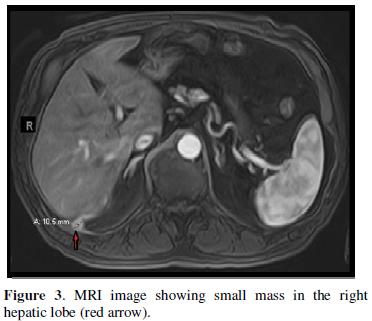
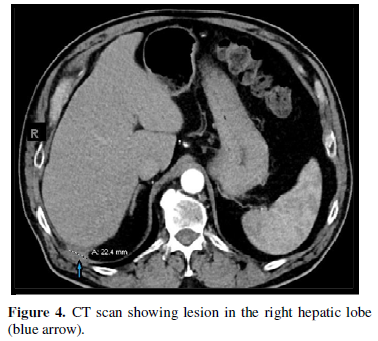
Traumatic brain injury is a leading cause of mortality and disability all over the world, most of skull fractures are simple and linear, compound depressed fractures follow. In this study, we have tried to predict depressed fracture associated injuries as Dural tear or Dural venous sinus injury preoperatively using head CT and MR venography. Dural repair is a neurosurgical procedure that requires a degree of experience, especially in cases where fractures are close to the skull base. For such cases, Dural tear may extend beyond the edge of the depressed segment to hardly approachable region [5]. The incidence of Dural tear ranged widely in literature, our study reported 26 % incidence of dural tear which is less than Gul Muhammad [6] with 33.7 %, Prakash [7] and Manne [8] with even higher incidence of 55 %. Similar to our results, Hossain [2] reported 25 % Dural tear incidence for all depressed fractures, while the highest incidence was reported by Nayak [3] with an incidence of 68 %, this wide variation is not explained to our knowledge. Cerebral contusions are a common associated pathology with depressed fracture which can be due to two mechanisms; direct due to impaction by blunt trauma, penetrating injury or sharp bone edge of the fracture. The other mechanism is hemorrhagic contusions secondary to compromised Dural venous sinus (Figure 4), a condition that requires surgical intervention to restore patency of the sinus [9] which highlights the importance of MRV study when sinus compression is suspected, as encountered in illustrative case (Figure 4). Epidural hematoma (EDH) in our study was found in 10 cases (21.7%), ranged from sizeable surgical EDH to small thin rim. To our knowledge, the highest incidence of depressed fracture associated EDH was reported by Satardey [10] with an incidence of 62 %. This vast variation of Dural tear and EDH incidence in literature can be attributed to the heterogeneity of the operative group among studies as well as discrepant indications of surgery throughout neurosurgical institutes. In this study pneumocephalus was subcategorized into three categories; parenchymal pneumocephalus, extra-axial at site of fracture and remote extra-axial. Dural tear was found in 100% of cases with parenchymal and remote pneumocephalus, which is hypothetically strong despite the limited number of cases of this study, this categorization is not included in Salia’s [11] formula. For example, applying Salia’s criteria [11] to illustrative case (Figure 3) of this study would give a low probability of dural tear in spite of radiological remote pneumocephalus which, to our results, is a sure sign of dural tear. Unlike remote and parenchymal pneumocephalus, local pneumocephalus alone was associated with dural tear in only 2/12 (16.7 %) of cases, which confirms that local pneumocephalus is mostly extradural and not a sign of dural tear. In a study by Salia [11], an algorism was concluded to predict dural tear preoperatively. Our results matched those of Salia [11] regarding cerebral contusion which was highly associated with dural tear group (60%) and the depth of depression which was 1.8 cm and 1.26 cm for torn and intact dura respectively in our study compared to 1.5 cm and 1 cm in Salia’s study. Another factor was included in this study, which is angulation of the depressed fracture, a correlation was found between higher angulation of the depressed segment and dural tear. To our knowledge, none of the previous study reported association between dural tear and angulation of the fracture, which is proven in this study that dural tears are to be related with higher angulation of the fracture in comparison to the intact dura group. Surgery for depressed fractures which are related to a dural venous sinus is a neurosurgical challenge, massive hemorrhage and air embolism are the main two intra-operative catastrophes to be avoided [12]. In this study, we classified dural venous sinus related fractures into two categories; direct which lies directly over the sinus, and near the sinus which are in the sinus vicinity without direct anatomical contact. Dural venous sinus direct involvement was found in 8 patients (17.4 %) which similar to Prakash and less than Rotterdam study [13] and Al Haddad [1], in our study only (50 %) of the fractures directly over a dural venous sinus were associated with sinus laceration that required repair according to intraoperative findings. In this study and literature, sinus injury and laceration was not predictable preoperatively, however sinus bleeding could be anticipated when epidural hematoma is related to a sinus(Figure 2), while sinus occlusion was preoperatively detected via MRV (Figure 4).The most common related dural sinus was superior sagittal sinus which is also the most common related sinus in Aziz [5], Meier [14], Meirowsky [15] and Kappa [16] with incidence of 70.6 %, 66 %, 557 % and 82 % among all sinus related depressed fractures respectively. Another parameter was added to this study is the proximity to the dural venous sinus i.e., depressed fractures near a dural venous sinus. Hypothetically; a depressed fracture indenting the dura would create epidural space forcibly enough to cause a dural venous sinus bleeding even for fractures which are not directly over to the sinus, this bleeding is noticed preoperatively on CT scan in the form of a rim of epidural hemorrhage, and intra-operatively by profuse bleeding below the bone edge related to the sinus, this bleeding is usually controlled by dural tucking. This was found in 8 of our patients (17.4 %) whose fractures were located 0.5-2 cm from the sinus. This encounter can be confirmed preoperatively by a thin rim of epidural hemorrhage extending between the fracture and the sinus (Figure 2) or prospected due to the proximity between the fracture and sinus, both conditions were reported in this study. This is an important pathology to be predicted preoperatively as some cases with profuse epidural bleeding from a dural venous sinus require blood transfusion especially in pediatric group. The main limitation of this study is its retrospective nature as well as the small number of cases in comparison to the prevalence of the pathology. Also, including cases which were managed conservatively might have added to the results, but the concept of the study was to compare preoperative scans to intra-operative findings.
CONCLUSION
Pathologies associated with depressed skull fractures are predictable with high accuracy, which is essential to prospect preoperatively to set up operative theater, surgical requirements and experience of the surgeon.
- Al-Haddad SA, Kirollos R (2002) A 5-year study of the outcome of surgically treated depressed skull fractures. Ann R Coll Surg Engl 84(3): 196-200.
- Hossain MZ, Mondle M, Hoque MM (1970) Depressed Skull Fracture: Outcome of Surgical Treatment. TAJ J Teach Assoc 21(2): 140-146.
- Nayak P, Mahapatra A (2008) Primary reconstruction of depressed skull fracture - The changing scenario. Indian J Neur 5(1): 35-38.
- Özer FD, Yurt A, Sucu HK, Tektaş Ş (2005) Depressed fractures over cranial venous sinus. J Emerg Med 29(2): 137-139.
- Aziz MM, El Molla ST, Abdelrahiem HA, Dawood OM (2019) Depressed skull fractures overlying dural venous sinuses: Management modalities and review of literature. Turk Neu 29(6) 856-863.
- Muhammad G, Aurangzeb A, Khan SA, Hussain I, Alam S, et al. (2017) Dural Tears in Patients with Depressed Skull Fractures. J Ayub Med Coll Abbottabad 29(2): 311-315.
- Prakash A, Harsh V, Gupta U, Kumar J, Kumar A (2018) Depressed fractures of skull: An institutional series of 453 patients and brief review of literature. Asian J Neu 13(2): 222.
- Manne S, Musali S, Gollapudi P, Nandigama P, Mohammed I, et al. (2019) Surgical outcomes in depressed skull fractures: An institutional experience. Asian J Neur 14(3): 815.
- Shao X, Wang Q, Shen J, Liu J, Chen S, et al. (2019) Treatment of Traumatic Depressed Compound Skull Fractures. J Craniofac Surg 30(7): 2239-2244.
- Satardey R, Balasubramaniam S, Pandya J, Mahey R (2018) Analysis of factors influencing outcome of depressed fracture of skull. Asian J Neur 13(2): 341.
- Salia SM, Mersha HB, Aklilu AT, Baleh AS, Lund-Johansen M (2018) Predicting Dural Tear in Compound Depressed Skull Fractures: A Prospective Multicenter Correlational Study. World Neur 114: e833-e839.
- LeFeuvre D, Taylor A, Peter JC (2004) Compound depressed skull fractures involving a venous sinus. Surg Neur 62(2): 121-125.
- Braakman R (1972) Depressed skull fracture: data, treatment, and follow-up in 225 consecutive cases. J Neur Neur Psy 1972;35(3):395-402.
- Meier U, Gärtner F, Knopf W, Klötzer R, Wolf O (1992) The traumatic dural sinus injury - a clinical study. Acta Neurochir (Wien) 119(1-4): 91-93.
- Meirowsky Am (1953) Wounds of dural sinuses. J Neurosurg 10(5): 496-514.
- Kapp JP, Gielchinsky I, Deardourff SL (1997) Operative techniques for management of lesions involving the dural venous sinuses. Surg Neurol 7(6): 339-342.
-
 Table 1
Table 1 -
Table 2








QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)


