2337
Views & Citations1337
Likes & Shares
Background: Tinnitus is defined as abnormal perception of sound without presence of any external sound. It can be treated by different audiological and non-audiological managements. Application based management of tinnitus is being accepted world-wide. However, this has many drawbacks. Therefore, there is a need to develop application-based management to overcome these difficulties.
Result: Wilcoxon sign rank test showed significant improvement in pre and post BTHI scores of each group. The Mann-Whitney U test showed significant difference in tinnitus pitch and loudness and no significant difference in post BTHI score between the two groups.
Conclusion: The study suggested that tinnitus masking through the developed android application is beneficial for all the age groups and due to its cost efficacy, it can be an economically viable option.
Keywords: Tinnitus, Tinnitus management, Tinni tool
NEED OF THE STUDY
There are various studies on tinnitus and tinnitus management [16]. Most of the studies on tinnitus management have focused on Tinnitus retraining therapy, various sound therapy techniques and effects of medications. Recent advances in gadget software’s have developed mobile applications which can be used in tinnitus management. Although masking noise through tinnitus masker provides some relief to the tinnitus sufferers [17] at the same time it also provides hindrance to communication performance Meikle, Griest, Stewart& Press (1995) [18]. Sabarish & Kruthika [19] have also reported the efficacy of android application for the treatment of tinnitus and the results revealed android based application could be used as a successive tool to reduce tinnitus which is cost effective and easily accessible by any individual. However, in Indian scenario, most of the people belong to a lower socio-economic stratum where they struggle with the primary needs of life like food habits, education, medical needs etc. Thus, in such a situation, tinnitus and its management take a backseat in their to-do list unless it becomes psychologically neurotic. For such a population, android application as a tinnitus-masking tool will prove to be both cost-effective and reliable. Because, if cost-effective tools cannot be provided for them, there will be a larger population deprived from tinnitus management and in cases of even starting management there will be more drop-outs. The goal of “Tinni tool” android application is to support both the hearing care professional (HCP) and patient with convenient access to tinnitus management because in India day by day there is increase in the use of smart phone users and thereby indirectly the tinnitus is also affecting the people but due to limited availability of audiologist in India, Several android app available in market were not standardized for tinnitus masker therefore standardization and development of appropriate android based application is required for tinnitus management. There are some commercially used device-based apps available in India based on two most popular smartphone platform play store and App store for the management of the tinnitus but they are very expensive and some are free apps but not used and liked much by the patients suffering from tinnitus because those aren’t enough flexible and multi parametric based to assess and manage tinnitus. There is also lack of evidence-based application for tinnitus that could highlight a need for research [10]. So, development of this app can be beneficial for use in day-to-day life by the tinnitus patients.
METHODS
In this present study Quasi Experimental research design was used. A total of 30 native Bengali speaking participants with complaint of tinnitus were included in the study (mean age 41.5, standard deviation 12.6) over a period of one year two months (January, 2019 to March, 2020). Participants were divided into two groups. Groups - I consisted of 15 participants (mean age 35.6, standard deviation 10.63) with the complaint of tinnitus with normal hearing sensitivity and Group - II consisted of 15 participants (mean age 47.4, standard deviation 12.04) with complaint of tinnitus with mild to moderate hearing loss. It was found that in Group I, 6 participants had tinnitus in left ear, 5 participants had tinnitus in right ear and 4 participants had tinnitus in both ears. However, in Group II, 5 participants had tinnitus in left ear, 4 participants in right ear and 6 participants in both ears.
The study was accomplished in following six stages:
Stage 1: Development of Tinnitus android application
Technical collaboration was established with the Meigionel Technology & Solutions OPC for development of application without any financial implication. Technical details were provided to the agency which included flow chart of application, requirement of pure tone and noise (Narrow Band Noise, Broad Band Noise, White Noise, Pink Noise, Violet Noise, and Speech Noise).
Criteria for inclusion & exclusion: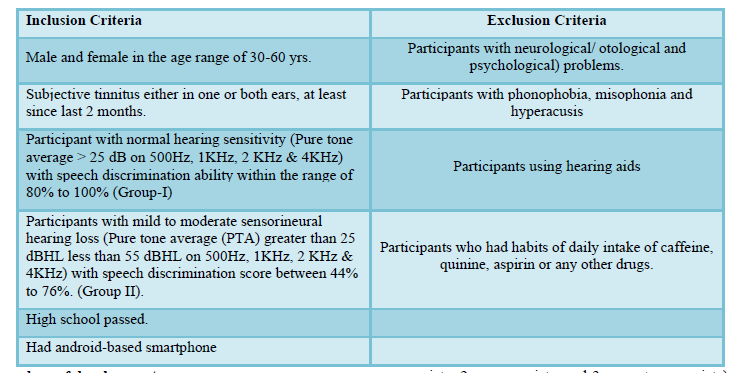
Procedure of development
“Tinni tool” a Tinnitus android application was developed through Integrated Development Environment (IDE) supported by IBM and Eclipse platform. Eclipse is popularly used for Java application development (Java SE and Java EE) and Android apps. It also supports PHP, C/C++, Perl, Python, and other web project developments through extensible plug-ins for individual profiling and analysis of the perceived tinnitus sound by a patient as well as for management. The developed android application contains 3 main modules - Pure tone audiometer, tinnitus sound generator and a tinnitus masker.
Stage 2: Objective and subjective validation of parameters of developed Tinnitus android application.
Objective Validation
Calibration: “Tinni tool” are finely calibrated & tested according to ANSI S3. 6-1989, ISO 389-1991, IEC 60645. Frequency Accuracy ±3% and Frequency Response ±3dB 125 - 4000 Hz and ±5dB 6000 & 8000 1989 (ANSI 1989 and ISO 1991).
Subjective validation
A questionnaire was prepared to assess the usefulness of developed application based on MAUQ (mHealth App Usability Questionnaire) which consist of 21 questions on three parameters (Ease of use and satisfaction, system information arrangement, and usefulness). Zhou, Bao, Setiawan, Saptono and Parmanto [20-22]. The above questionnaire was modified to suit the need of the study in such a way that modified questionnaire consists of a total of 17 questions. The questionnaire was given to 10 audiologists to rate the content on three-point rating scale (1 = not appropriate, 2 = appropriate, and 3 = most appropriate) and suggestion, if any modification or changes are required in the application. Positive feedback was obtained from all the audiologists regarding appropriateness of “Tinni tool” on the basis of ease of usage and satisfaction, system information arrangement and its usefulness. The result showed good inter-judge agreement (r = 0.86) between the appropriate and most appropriate rating given by 10 judges.
Stage 3: Participant selection
The participants were selected from the Audiology Department of AYJNISHD, RC, Kolkata fulfilling the inclusion criteria of the study & were explained about the purpose of the study before obtaining written Consent.
Stage 4: Assessment of tinnitus
A detailed case history including the demographic data, medical history, family history, educational history and economic background of the participants were taken. Case history information included significant history like vertigo, aural fullness, pressure fluctuations within the ear, fluctuations in hearing, ear pain or discomfort, tinnitus and other physical complain. This information was obtained to understand the lifestyle, know about the problem and needs of the patients. After recording relevant information, the participants underwent an audiological evaluation including otoscopic examination, pure tone audiometry, tympanometry and speech recognition thresholds. Otoscopic examination was performed routinely prior to check the presence of cerumen or any sign of infection in the external auditory canal or furuncle. The visibility of the tympanic membrane was noticed during otoscopic examination. Tinnitus Handicap Inventory in Bangla [23] (B-THI) was used to assess the participant’s perceived severity of tinnitus. The B-THI is a self-administered, 25 – item questionnaire that is scored on a 3-point scale (No = 0, Sometimes = 2 and Yes =4). The total THI score is the sum of the scores for the following three subclasses: functional, emotional and catastrophic. Psychoacoustic assessment was done for all the participants. Tinnitus pitch and loudness were matched using procedure given by Henry and Zaugg [24]. Tinnitus matching was done using Resonance r37 audiometer. Along with this Minimal masking level (MML) procedure & Residual Inhibition test was administered. The outcomes were measured in three ways; positive-complete, positive-partial, negative or rebound. Only positive-complete and positive-partial were considered among all of these categories.
Stage 5: Intervention of Tinnitus using developed android application “Tinni Tool”
Therapeutic protocol: All participants were administered tinnitus masking at the level of MML + 20 dB at matched-frequency to the tinnitus in the ipsilateral ear. Stimulus was selected as matched through psychoacoustic assessment & was generated by developed “Tinni tool” with Ear phone. Intensity and frequency of masking stimulus was controlled by up and down button. All the participants have given minimal instruction and no counselling and also given tinnitus masking for 30 minutes daily and 3 times in a day. They were asked to use the “Tinni tool” application at home on their smartphone & regular feedback was taken weekly about his/her tinnitus problem through telephonic conversation. If the participant faced any kind of problem they were be asked to visit the Institution.
Stage 6: Validation of the same application
The therapy was terminated when the tinnitus disappeared with maximum duration of two month. The same standardized method as used during the pre-therapy were used to assess post therapy effects of the participants.
Stage 7: Statistical analysis
All the data were tabulated in MS office 2010 Excel data sheet and statistical analyses (Shapiro Wilks test of normality & Wilcoxon signed ranks test) were performed using the software package of social science (SPSS) software version 20.0.
RESULTS
The purpose of the present study was to develop android based application named “Tinni tool” and to verify the accuracy of the acoustic output of “Tinni tool” using sound level meter and frequency counter. Another objective of the study was to validate the application in clinical population. Furthermore, Shapiro-wilk’s test was done to assess the normality of data for both pre and post scores of B-THI, tinnitus pitch, and tinnitus loudness in Group I and Group II. As Shapiro-Wilk test indicated that pre and post scores of B-THI, tinnitus pitch, and tinnitus loudness scores were not normally distributed (p < 0.05) therefore, a non-parametric test, Wilcoxon Signed Ranks Test was done to evaluate the data objectively (Table 1).
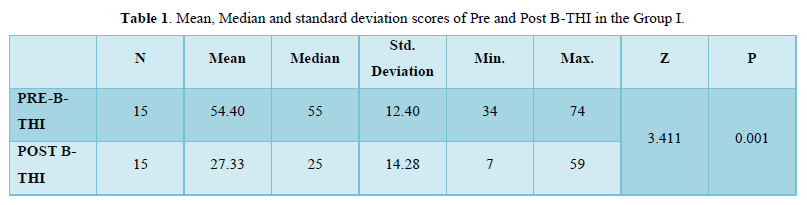
The present study revealed significant differences (Z= 3.411; p = .001) in Group I participants on B-THI scores for pre and post condition in all the three domains (functional, emotional and catastrophic) after intervention through “Tinni Tool” (Table 2).

Table 2 also showed significant difference (Z= 2.54; p = 0.0001) between pre and post tinnitus pitch value in Group I participants.
Changes of the loudness in Table 3 also indicated significant difference (Z= 3.632; p = .0000) between pre and post tinnitus loudness value in Group I participants.

The present study revealed significant differences (Z= 3.412; p = 0.0001) in Group II participants on B-THI scores in pre and post condition with improvement in all the three domains (functional, emotional, catastrophic) after use of “Tinni Tool” (Table4).
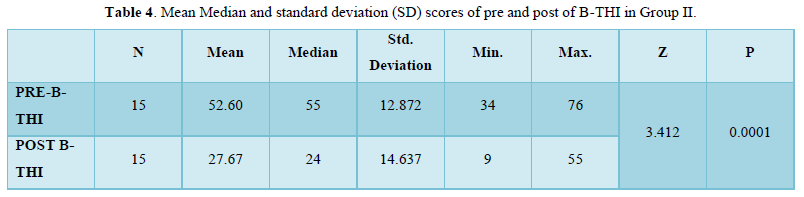
Table 5 depicted significant difference (Z= 3.058; p = 0.0002) between pre and post tinnitus pitch value in Group II participants.

Table 6 revealed significant difference (Z= 4.18; p = 0.000) between pre and post tinnitus loudness value in Group II participants.

The findings of present study revealed no significant difference (Z= 0.187; p = 0.870) between the scores of B-THI in Group I and Group II participants (Table 7).

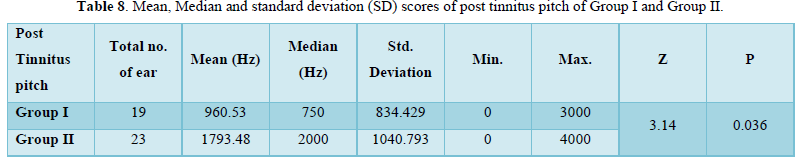
The results also indicated significant difference between (Z= 3.41; p = 0.036) the scores of tinnitus pitch between Group I and Group II participants (Table 8).
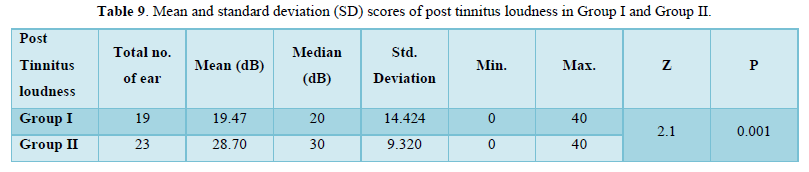
The present findings revealed significant difference (Z= 2.1; p = 0.001) between the scores of tinnitus loudness between Group I and Group II participants (Table 9).
DISCUSSION
The present study indicated that the severity of tinnitus was reduced after using “Tinni tool” for both the groups. The present findings agree with study undertaken by Sabarish and Kruthika [19] who reported reduction in the severity of tinnitus to 25-30% with the decrease in scores of THI in comparison to pre-therapy when intervened using different sounds presented through different android applications. Another study supporting the present finding has been conducted by Sarac and Arli [20]. They reported low THI score after Tinnitus masking treatment (TMT) using audiometer in patients having tinnitus with hearing loss. In addition to this, the functional aspects such as concentration, physical & occupational functioning was improved and emotional aspects such as anxiety, depression, frustration, anger was reduced after tinnitus masking due to suppression of tinnitus [21-22]. It is also found out that after usage of “Tinni tool” there is shifting in the pitch towards the lower range in both the groups may be due to off-frequency listening. This is in consonance with study of Weisz, Hartmann, Dohrmann, Schlee, and Norena [23]. They reported shifting of pitch from higher to lower frequency (for off-frequency listening) when stimuli were presented in a region of severely damaged inner-hair cells, as the information were provided from the neighboring regions i.e. from less or undamaged regions. When the tone is presented above the threshold level, it caused the various neighboring auditory filters to contribute to the output and thus leads to frequency shifting [24]. However, this finding may be interpreted cautiously. The loudness reduction in the post therapy condition for both the groups as compared to pre-therapy condition using “Tinni tool” proved to be an indicator that the masking noise provided by “Tinni tool” was sufficient to suppress tinnitus. This finding agreed with the findings of Vernon and Meikle [25] who reported significant reduction in the loudness and severity of tinnitus after taking Alprazolam, though the mode of intervention was different. Another study supporting the present finding was done by Okamoto, Stracke, Stoll, and Pantev [26]. Authors reported that tinnitus loudness was significantly diminished using custom-tailored notched music treatment due to reduced cortical activity corresponding to notched center frequency possibly through the process of lateral inhibition. So, it may be inferred that the suppression of the tinnitus loudness in the present study can be due to lateral inhibition. Lateral inhibition is generally referred to as the capacity of an excited neuron to reduce the activity of its neighbors. However, this finding too interpreted cautiously. The study also showed that there is no significant difference in perceived tinnitus handicap on total THI and its subscales between subjects with normal hearing and those with hearing loss agreed with result of Newman, Jacobson, and Spitzer [6] & Lim, Lu, Koh, and Eng [27]. They reported no significant difference in the overall THI and subscale scores in patients with or without hearing loss, and those with unilateral or bilateral tinnitus. But it is found out that the pitch of the tinnitus is significantly different between the groups. These findings are in consonance with result of Martines, Bentivegna, Martines, Sciacca, and Martinciglio [28] who reported significant difference between two groups (groups konsa). They concluded that tinnitus pitch differs in the hearing loss and normal hearing group because of association between high-pitched tinnitus and high-frequency sensorineural hearing loss. Further, it was also suggested that hearing loss led to auditory pathway reorganization and this could be one of the main sources of tinnitus sensation more in participants of Group II. The reduction of loudness is more in Group I as compared to Group II this might be due to the fact that neural synchrony hypothesis predicts the tinnitus spectra, and so far, unmeasured “residual inhibition functions” that relate residual tinnitus suppression to the center frequency masking sound should cover the region of hearing loss in the audiogram. Residual inhibition depth was shallower when the masking sounds that were used to induce residual inhibition showed decreased correspondence with the frequency spectrum and bandwidth to the tinnitus. These findings suggested that tinnitus and its suppression inhibition depend on processes that span the region of hearing impairment and not on mechanisms that enhance cortical representation for sound frequency at the audiometric edge reported by Roberts, Mofeat, Baumann, Ward, and Bosnyak [29]. Although this study suggested that the development of “Tinni tool” is an effective android application for tinnitus management still it needs to be studied with different noises (white noise, pink noise, violet noise and speech noise) for measurement of treatment efficacy and also the comparison study should be done with other android applications.
CONCLUSION
Hence, the study provides a structured temporal course for providing tinnitus masking therapy for tinnitus with normal hearing participants as well as for tinnitus with mild to moderate sensorineural hearing loss. Although tinnitus masking is a critical element for tinnitus treatment and the results suggest that developed android application “Tinni tool” can be used as noise generator for effective tinnitus masking with reference to its cost efficacy and it can be an economically viable option for distant patients.
- McFadden D (1982) Tinnitus: Facts, theories, and treatments. Washington, DC: National Academies Press, pp: 1-7.
- Vernon JA, Fenwick J (1984) Identification of tinnitus: A plea for standardization. J Laryngol Otol 98(S9): 45-33.
- Moller A (2000) Similarities between severe tinnitus and chronic pain. J Am Acad Audiol 11: 115-124.
- Coles RRA, Baskill JL, Sheldrake JB (1985) Measurement and management of tinnitus part II. Management. J Laryngol Otol 99(1): 1-10.
- Halford J, Anderson SD (1991) Tinnitus severity measured by a subjective scale, audiometry and clinical judgement. J Laryngol Otol 105(2): 89-93.
- Newman CW, Jacobson GP, Spitzer JB (1996) Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg 122: 143-148.
- Henry JA, Zaugg TL, Schechter MA (2005a) Clinical guide for Audiologic Tinnitus Management I: Assessment. Am J Audiol 14: 21-48.
- Henry JA, Zaugg TL, Schechter MA (2005b) Clinical guide for Audiologic Tinnitus Management II: Treatment. Am J Audiol 14: 49-70.
- Henry JA, Zaugg TL, Myers PJ, Schechter MA (2008) Using therapeutic sound with Progressive Audiologic Tinnitus Management. Trends Amplif 12: 188-209.
- Wise K, Ma E (2016) Clinical Presentation of Tinnitus and a Review of, and Evidence Base for, Tinnitus Applications. Perspect ASHA SIGs 1(7): 43-56.
- Vernon J (1977) Attempts to relieve tinnitus. J Am Audiol Soc 2(4): 124-131.
- Vernon JA (1988) Current use of masking for the relief of tinnitus. In: Kitahara M, ed. Tinnitus. Pathophysiology and Management. Tokyo: Igaku-Shoin pp: 96-106.
- Bo LD, Ambrosetti U (2007) Hearing aids for the treatment of tinnitus. Prog Brain Res 166: 341-345.
- Folmer RL, Carroll JR (2006) Long-term effectiveness of ear-level devices for tinnitus. Otolaryngol Head Neck Surg 134(1): 132-137.
- Henry JA, Schechter MA, Zaugg, TL, Griest S, Jastreboff PJ, et al. (2006) Clinical trial to compare tinnitus masking and tinnitus retraining therapy. Acta Oto-Laryngologica 126(sup556): 64-69.
- Newman CW, Sandridge SA (2012) A comparison of benefit and economic value between two sound therapy tinnitus management options. J Am Acad Audiol 23(2): 126-138.
- Mitchell C (1983) The masking of tinnitus with pure tones. Audiology 22(1): 73-87.
- Meikle MB, Griest SE, Stewart BJ, Press LS (1995) Measuring the negative impact of tinnitus: A brief severity index. In Abstract Association for Research in Otolaryngology pp: 167.
- Sabarish A, Kruthika S (2019) Efficacy of sound therapy using android based application in individual with tinnitus.
- Sarac ET, Arli C (2018) Effects of tinnitus masking therapy in tinnitus patients with and without hearing loss. JTMC 25(2): 222-224
- Hazell JWP, Wood SM (1981) Tinnitus masking-a significant contribution to tinnitus management. Br J Audiol 15(4): 223-230.
- Sandlin RE, Olsson RJ (1999) Evaluation and selection of maskers and other devices used in the treatment of tinnitus and hyperacusis. Trends Amplif 4(1): 6-26.
- Weisz N, Hartmann T, Dohrmann K, Schlee W, Norena A (2006) High-frequency tinnitus without hearing loss does not mean absence of differentiation. Hear Res 222(1-2): 108-114.
- Moore BC (2010) The relationship between tinnitus pitch and the edge frequency of the audiogram in individuals with hearing impairment and tonal tinnitus. Hear Res 261(1-2): 51-56.
- Vernon, JA, Meikle MB (2003) Tinnitus: Clinical measurement. Otolaryngol Clin North Am 36(2): 293-305.
- Okamoto H, Stracke H, Stoll W, Pantev C (2010) Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity. Proceed Nat Acad Sci 107(3): 1207-1210.
- Lim JJBH, Lu PKS, Koh DSQ, Eng SP (2010) Impact of tinnitus as measured by the Tinnitus Handicap Inventory among tinnitus sufferers in Singapore. Sing Med J 51(7): 551-557.
- Martines F, Bentivegna D, Martines E, Sciacca V, Martinciglio G (2010) Characteristics of tinnitus with or without hearing loss: Clinical observations in Sicilian tinnitus patients. Auris Nasus Larynx 37(6): 685-693.
- Roberts LE, Moffat G, Baumann M, Ward LM, Bosnyak DJ (2008) Residual inhibition functions overlap tinnitus spectra and the region of auditory threshold shift. J Assoc Res Otolaryngol 9(4): 417-435.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
-
Table 9









QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Pathology and Toxicology Research
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)


