2
Views & Citations10
Likes & Shares
Histologically, the gallbladder wall is divided into the three layers: (1) mucosa, (2) muscular layer, and subserosa. The mucosa is subdivided into the two components: the columnar epithelium, and lamina propria mucosae. The muscular layer consists of the thin layer of smooth muscle bundles. The subserosa is composed of loose connective tissue, including medium-sized arteries/veins/nerves.
There are small tubulo-alveolar glands in the wall of the gallbladder neck and the cystic duct. The gallbladder wall frequently shows Rokitansky-Aschoff sinuses which are diverticulum-like structure of mucosal epithelium into and through the muscular layer.
ANOMALOUS PANCREATICOBILIARY DUCTAL UNION (APBDU)
In the APBDU cases, the junction of the common bile duct and pancreatic duct lies outside the duodenal wall (sphincter of Oddi) and is frequently associated with congenital choledochal cyst/dilatation [2]. The gallbladder with APBDU shows mucosal hyperplasia, one of the high-risk lesions of gallbladder adenocarcinoma.
CHOLESTEROLOSIS
Cholesterolosis refers to lipid deposition within macrophages in the lamina propria mucosae and is one of the most common diseases of gallbladder (Figure 1). Macroscopically, the gallbladder mucosa shows granular or reticular pattern of cholesterolosis in golden-yellow to white-yellow color. Microscopically, numerous lipid-laden macrophages aggregate in the lamina propria mucosae.
- Acute cholecystitis
Acute cholecystitis is caused by inflammation, blood circular disturbance such as ischemia, and chemicals. The gallbladder wall exhibits mucosal edema, congestion/hemorrhage, and erosion. Edema, congestion/hemorrhage, fibrinous exudates are associated with ischemic changes, and inflammatory cells such as neutrophils are related to the infection.
A-1. Acute gangrenous cholecystitis
Acute gangrenous cholecystitis is caused by circular disturbance, and characterized by extensive transmural necrosis with edema, congestion/hemorrhage, erosion/ulceration, and inflammatory exudates. Transmural ghost-like necrosis is caused by severe ischemia and infarction.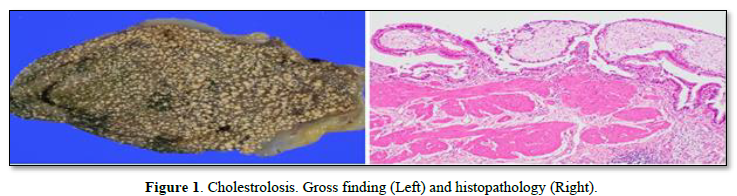
INFLAMMATION
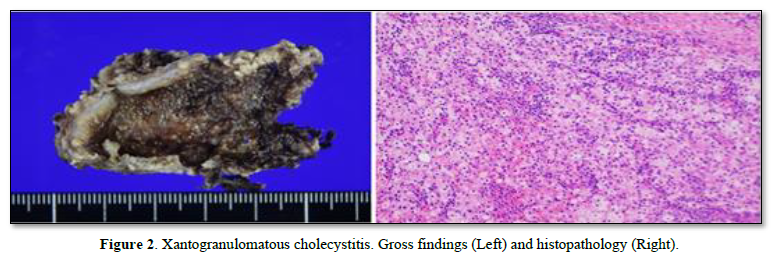
A-2. Xanthogranulomatous cholecystitis (XGC)
XGC is a rare type of gallbladder inflammation and is characterized by xanthogranuloma formation with lipid-laden macrophages and granulation tissue. XGC occasionally forms pseudo-tumoral lesion with adjacent organ involvement, mimicking gallbladder cancer (Figure 2).
- Chronic cholecystitis
Chronic cholecystitis results from chronic persistent inflammation of the gallstones, and/or prolonged state of acute cholecystitis. Histologically, chronic cholecystitis is characterized by (1) inflammatory cell infiltration occasionally with lymphoid follicle formation, (2) fibrosis with gallbladder wall thickening, and (3) changes of mucosal epithelium frequently with metaplasia.
B-1. Metaplasia
Various metaplastic changes are present in gallbladder mucosa, including pyloric gland metaplasia (gastric metaplasia), goblet cell metaplasia (intestinal metaplasia), and surface cell mucous metaplasia (Figure 3) [3].
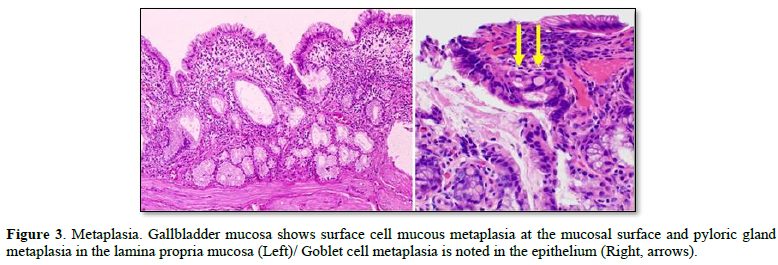
Pyloric gland metaplasia, also known as gastric metaplasia, results from chronic inflammation and forms tubule-alveolar mucous glands similar to the gastric pyloric glands. Goblet cell metaplasia, also intestinal metaplasia, is characterized by goblet cells in the mucosal epithelium. Intestinal metaplasia is infrequently associated with Paneth cell and brush border formation.
Immunohistochemically, the gallbladder epithelium without metaplasia is positive for CD10 and CA19-9 at the epithelial luminal surface. MUC5AC-positive cells are present at the mucosal surface epithelium with pyloric gland metaplasia and/or surface cell mucous metaplasia. In addition, MUC-6 immunoreactivity is noted in the metaplastic pyloric glands. Intestinal metaplasia shows MUC2-positive goblet cells in the epithelium.
TUMOR-LIKE LESIONS, INCLUDING ADENOMYOMATOSIS AND POLYPS
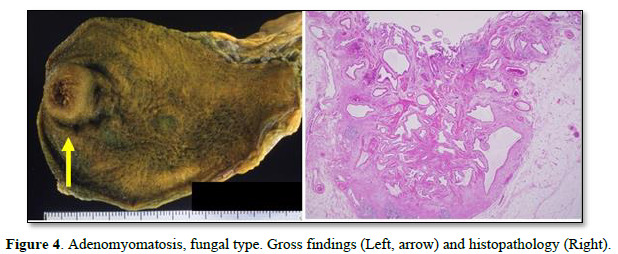
- Adenomyomatosis
Adenomyomatosis, also known as adenomyomatous hyperplasia, is hyperplastic changes of Rokitansky-Aschoff sinuses in the gallbladder wall, frequently related to fibromuscular thickening of gallbladder wall (Figure 4) [3]. Macroscopically, adenomyomatosis is usually divided into three types. (1) fundal type (local type), adenomyomatosis forms a tumorous lesion mimicking true neoplasia; (2) segmental type (annular type), adenomyomatosis deforms the gallbladder in an hourglass-like shape; and (3) diffuse type.
- Polyps
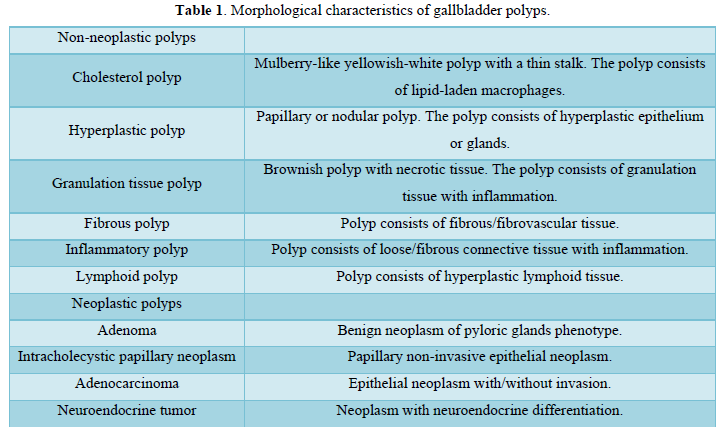
Gallbladder polypoid lesions include neoplastic lesions such as adenoma and adenocarcinoma (intramucosal), and non-neoplastic polyps such as cholesterol polyp, hyperplastic polyp, and granulation tissue polyps (Figure 5) [3].
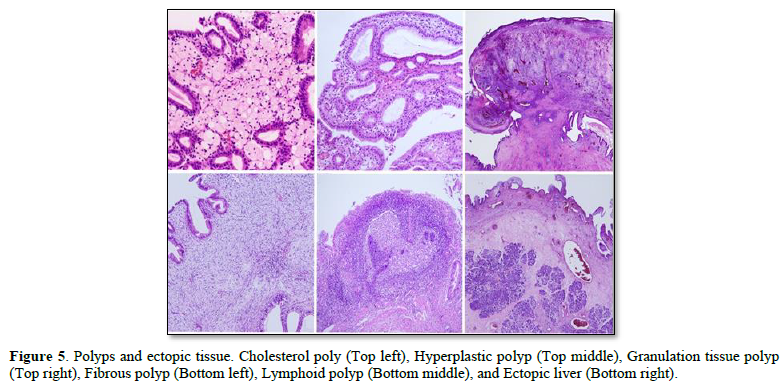
Cholesterol polyp is the most common type of gallbladder polyps and is characterized by lipid-laden macrophages and hyperplastic epithelium. Hyperplastic polyp consists of epithelial or glandular hyperplasia without atypia. Granulation tissue consists of granulation tissue with inflammation and is frequently related to the acute cholecystitis. Fibrous polyp and inflammatory polyp are composed of loose connective tissue and are associated with resolving stage of acute inflammation. Lymphoid polyp consists of hyperplastic lymphoid tissue with germinal centers (Table 1).
- Ectopic tissues
Several types of ectopic tissue, such as liver, pancreas, and gastric mucosa, are noted in and attached to the gallbladder wall.
TUMORS
The most of gallbladder tumors are epithelial neoplasms and are divided into the three categories: benign epithelial tumors, borderline epithelial tumors (precursors), and malignant epithelial tumors [4] (Table 2).
- Benign epithelial tumor
A-1. Pyloric gland adenoma
Pyloric gland adenoma is recognized as nodular polyp and is histologically composed of packed small pyloric-type glands with minimal stroma [3,5]. MUC-6 immunoreactivity is noted in the pyloric-type glands.
- Borderline epithelial tumor (precursors)
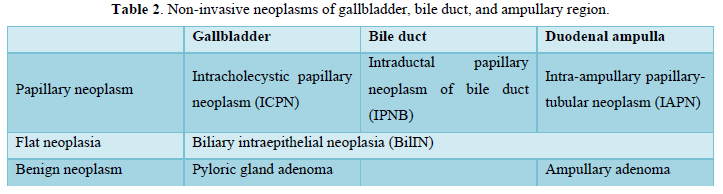
Borderline epithelial tumors are classified as the two categories: intracholecystic papillary neoplasm (ICPN) and biliary intraepithelial neoplasia (BilIN).
B-1. Intracholecystic papillary neoplasm (ICPN)
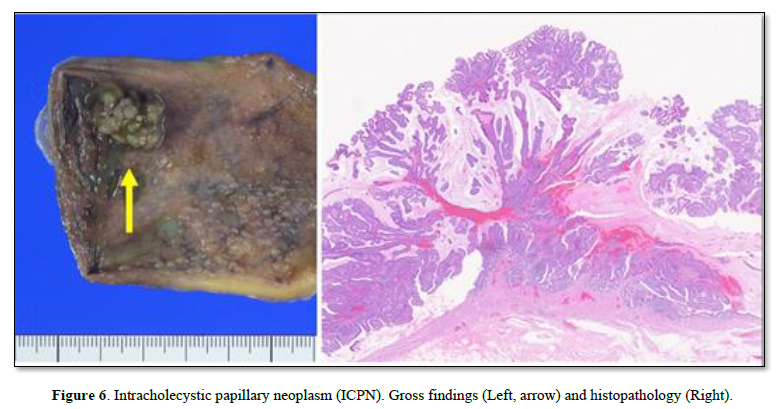
ICPN is grossly recognized as mass forming, non-invasive epithelial neoplasm arising from the gallbladder lumen (Figure 6). ICPN forms an exophytic (papillary or polypoid) company lesion, frequently more than 1 cm in a size [4,6]. According to the histopathological findings, ICPN is divided into the three groups: ICPN with low-grade intraepithelial neoplasia, ICPN with high-grade intraepithelial neoplasia, and ICPN with associated with invasive carcinoma. Four morphological phenotypes are recognized: (1) biliary type (frequently positive for CK7, MUC1), (2) gastric type (frequently positive for MUC5AC, MUC6), (3) intestinal type (frequently positive for CK20, CDX2, MUC2), and (4) oncocytic type (rare).
B-2. Biliary intraepithelial neoplasia (BilIN)
BilIN is microscopically recognized as non-invasive flat (or micropapillary) neoplastic lesion of gallbladder lumen [3, 4]. According to the histopathological atypia, BilIN is divided into the two groups: low-grade BilIN and high-grade BilIN. High-grade BilIN shows neoplastic atypia with nuclear pleomorphism. Differential diagnosis between low-grade BilIN and reactive epithelial atypia, as well as differential diagnosis between high-grade BilIN and carcinoma in situ, are difficult.
- Malignant epithelial tumor
C-1. Adenocarcinoma
Adenocarcinoma is the most common histological type of gallbladder carcinoma [3]. The adenocarcinomas frequently show invasive growth in the gallbladder wall, characterized by well differentiated type at the superficial part of tumor, and moderately to poorly differentiated type at the invasive front of tumor. The invasive carcinoma induces stromal desmoplasia (irregular fibrosis) in the gallbladder wall and is associated with frequent lymphatic/venous/perineural invasion [7-9].
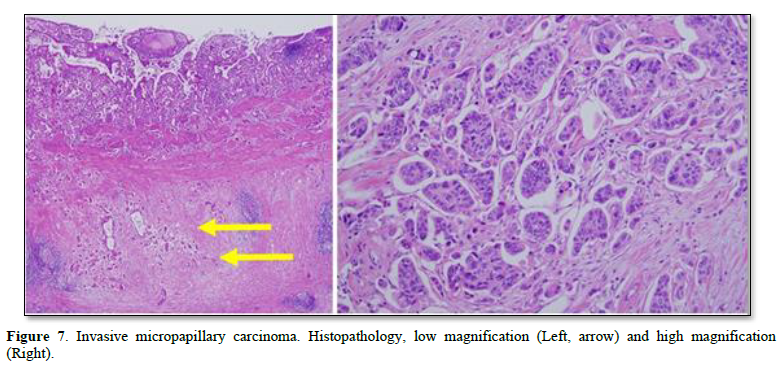
The various patterns of adenocarcinoma are noted as follows: biliary-type adenocarcinoma (frequently positive for CK7, MUC1), intestinal-type adenocarcinoma (frequently positive for CK20, CDX2, MUC2), gastric-type adenocarcinoma (frequently positive for MUC5AC, MUC6), and mucinous adenocarcinoma [10, 11]. Invasive micropapillary carcinoma (IMPC) is one of the specific adenocarcinomas with aggressive clinicopathological behavior and is characterized by micropapillary clusters within clear stromal spaces (Figure 7) [12]. The clusters are composed of tumor cells with pleomorphic nuclei.
C-2. Adenosquamous carcinoma, Squamous cell carcinoma
Adenosquamous carcinoma consists of two substantial components (more than 25% of tumor): adenocarcinoma part, and squamous cell carcinoma part. Pure squamous cell carcinoma is rare and shows aggressive behavior.
C-3. Undifferentiated carcinoma
Undifferentiated carcinoma is rare and has non-glandular, non-descript morphology with high cellular pleomorphism.
C-4. Neuroeodocrine neoplasm (NEN)
Neuroendocrine neoplasm (NEN) is divided into the two categories: neuroendocrine tumor (NET), and neuroendocrine carcinoma (NEC) [4]. NET consists of tumor cells with well differentiated endocrine phenotype and is graded as G1, G2, and G3. NEC is composed of carcinoma cells with poorly differentiated endocrine phenotype and subdivided into the small cell type SCNEC), and large cell type (LCNEC). Many cases of NEC have non-neuroendocrine component such as adenocarcinoma and are recognized as mixed neuroendocrine - non-neuroendocrine neoplasm (MiNEN).
ACKNOWLEDGEMENTS
This study was supported by JSPS KAKENHI, Grants-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
- Millis, SE (ed.). (2020) Histology for pathologists. 5th Wolters Kluwer, Philadelphia.
- Lack EE (2003) Pathology of the pancreas, gallbladder, extrahepatic biliary tract, and ampullary region. Oxford, New York.
- Albores-Saavedra J, Henson DE, Klimstra DS (2015) Tumors of the gallbladder, extrahepatic bile ducts and ampulla of Vater. Atlas of tumor pathology. 4th series, fascicle 23. Armed Forces Institute of Pathology (AFIP), Washington DC.
- WHO (2019) WHO classification of tumors editorial board (ed.). WHO classification of tumours. 5th edition. Digestive system. IARC, Lyon.
- Kijima H, Watanabe H, Iwafuchi M, Ishihara N (1989) Histogenesis of gallbladder carcinoma from investigation of early carcinoma and microcarcinoma. Acta Pathol Jpn 39: 235-244.
- Adsay V, Jang KT, Roa JC, Dursun N, Ohike N, et al. (2012) Intracholecystic papillary-tubular neoplasms (ICPN) of the gallbladder (neoplastic polyps, adenomas, and papillary neoplasms that are ≥1.0 cm): clinicopathologic and immunohistochemical analysis of 123 cases. Am J Surg Pathol 36: 1279-1301.
- Kijima H, Wu Y, Yoshizawa T, Suzuki T, Tsugeno Y, et al. (2014) Pathological characteristics of early to advanced gallbladder carcinoma and extrahepatic cholangiocarcinoma. J Hepatobiliary Pancreat Sci 21: 453-458.
- Nagino M, Hirano S, Yoshitomi H, Aoki T, Uesaka K, et al. (2021) Clinical practice guidelines for the management of biliary tract cancers 2019: The 3rd English edition. J Hepatobiliary Pancreat Sci 28: 26-54.
- Okada K, Kijima H, Imaizumi T, Hirabayashi K, Matsuyama M, et al. (2012) Clinical significance of wall invasion pattern of subserosa-invasive gallbladder carcinoma. Oncol Rep 28: 1531-1536.
- Kashiwagi H, Kijima H, Dowaki S, Ohtani Y, Tobita K, et al. (2000) DF3 expression in human gallbladder carcinoma: significance for lymphatic invasion. Int J Oncol 16: 455-459.
- Kashiwagi H, Kijima H, Dowaki S, Ohtani Y, Tobita K, et al. (2001) MUC1 and MUC2 expression in human gallbladder carcinoma: a clinicopathological study and relationship with prognosis. Oncol Rep 8: 485-489.
- Hara S, Kijima H, Okada K, Igarashi Y (2010) Invasive micropapillary variant of the gallbladder adenocarcinoma and its aggressive potential for lymph node metastasis. Biomed Res 31: 89-95.
-
 Table 1
Table 1 -
Table 2









QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)


