Journal of Ageing and Restorative Medicine (ISSN:2637-7403)

Research Article
Association Between Cardiovascular Risk Factors and Nutritional Status in Primary Care Users in a Health Unit
6272
Views & Citations5272
Likes & Shares
Introduction: Being characterized as a multifactorial pathology, complex and difficult to identify its cause. Anthropometric indicators are known to be a good tool for assessing nutritional status, which has been widely used in research because it is a cheap, innocuous and simple method to perform.
Objective: To evaluate the association between cardiovascular risk factors and nutritional status in Primary Care users at a Health Unit in São Luís, MA.
Method: This is a cross-sectional study focused on assessing cardiovascular risk by anthropometry and achieving cost-effective results for participants' health. The sample was non-probabilistic and composed by 171 patients of both sexes, aged ≥ 18 years and with co-morbidities, linked to a Basic Health Unit of São Luís, MA.
Results: The study showed a predominance of overweight people (n = 131) both sexes, self-declared color non-white (84.73%), non-smokers (89.3%) non-alcoholic (79.4%) prevalence. in both groups (eutrophic and overweight) sedentary people 82.5% and 79.4%, respectively. The evaluation of body composition and hemodynamic indicators showed alteration of all measurements in both groups. And the regression-adjusted analysis of body composition and hemodynamic measurements showed statistically significant results only for waist circumference (<0.001) and conicity index (<0.001).
Conclusion: Knowing the profile of the population in which we are working to observe the priority needs and designing effective and safe interventions within the reality of each scenario is fundamental to improve quality of health and life of individuals.
Keywords: Anthropometry, Overweight, Diabetes, Hypertension
INTRODUCTION
Overweight and obesity are characterized by an increase in body fat resulting from the imbalance between food intake and caloric expenditure [1-3].
Also, obesity is recognized worldwide as a multifactorial disease, complex and difficult to identify its cause, since there are several factors involved in the process that can somehow interfere in the development of overweight in the individual, as these have: physiological, genetic, psychological, environmental, cultural and behavioral factors [4].
According to the World Health Organization (WHO), the projection is that in 2025, about 2.3 billion adults are overweight, and more than 700 million are obese. In Brazil, obesity is growing more and more, and the latest data released by the Brazilian Institute of Geography and Statistics (IBGE), was in the period 2008-2009 [5]. In the North east region, overweight in adults was 44.45%. The Brazilian Association for the Study of Obesity and Metabolic Syndrome (ABESO) has the purpose of maintaining an updated map on the website, on the prevalence of obesity from official information for each region.
The relationship between the development of cardiovascular diseases and modifiable and non-modifiable risk factors is well established. And when it comes to body composition, some prospective studies have examined its relationship with cardiovascular diseases, has found a direct association between both [4,6]. In the current scenario, cardiovascular diseases are recognized as entities of multifactorial origin have been responsible for high rates of morbidity and mortality in Brazil and in the world [7-9]. It is noteworthy that in Brazil about one-third of deaths from CVD are occurring in adults between the age group of 35 to 64 years old [10,11].
Obesity is still recognized as one of the biggest risk factors for the development of insulin resistance (IR) and the accumulation of lipids in the muscles and in the visceral cavity is an aggravating factor for the development of metabolic syndrome (MS), as well as insulin resistance itself; which can increase the risk for several diseases such as dyslipidemia, hypertension, reduced glucose tolerance, type 2 diabetes mellitus, and fatty liver [12].
Given this scenario, making an early diagnosis of nutritional status is essential for the design of positive intervention strategies in the scope of primary and secondary prevention. One of the most used methods in the assessment of body composition is anthropometry for its good reproducibility, simplicity, for being innocuous a do flow cost, which can still be applied in a largen number of individuals; in addition to being relatively easy to interpret and being effective in assessing cardiovascular risk [13-15].
The assessment of cardiovascular risk factors should be applied because it is a relevant measure to define therapeutic approaches by professionals working in public health, especially those in the Family Health Strategy (SHF). It is also important in directing health prevention and promotion actions, assistance to the most prevalence diseases, health recovery, and rehabilitation [16].
In this context, this study aimed to assess the association between cardiovascular risk factor sand nutritional status in Primary Care user sat a Health Unit in São Luís, MA.
METHODS
The research model used in this study was the cross-sectional design, carried out in the area covered by the Family Health Unit (USF) Antônio Guanaré, in the Coroadinho neighborhood, in the municipality of São Luís, State of Maranhão, Brazil. The research was carried out from August 2015 to December 2016.
The sample calculation allowed determining a sample of 171 users. The following estimates were used: the total number of people registered in the e-SUS AB of the Family Health Strategy of UBS Antônio Guanaré is: 285; Prevails mean in the population are overweight and 51% are Luí s 46%; Sampling error: 5%; Confidence interval: 95%. Thus, the calculated sample was 156, plus 10% for possible losses or refusals, totaling 171 participants. The Brazilian average was used for the calculation.
All users who met the following criteria were included in the research: Age ≥ 18 years; attend UBS regularly (at least once a month); have comorbidities. The volunteers who signed the Free and Informed Consent Form (ICF), after due explanation and who met the inclusion criteria were selected. Will include inclusion will be used: to have cognitive impairment that prevented them from understanding and responding to the forms and informed consent; be institutionalized (hospitalized, asylum or with freedom in a private state) at the time of the information collection procedure through the application of the form (script).
Data collection was performed using the direct observation technique and the Pharmaceutical Care Guide proposed by the Pharmaceutical Care Booklet of the Ministry of Health (2014), adapted. The method comprised the following steps: invitation to participate in the study, study phase and situational analysis; and global health assessment.
The form was aimed at investigating the following variables: self-reported color, regular physical activity (at least 03 times/week), consumption of alcoholic beverages, smoking (the consumption of at least one cigarette in the last month was considered as such), systemic arterial hypertension (HAS), diabetes mellitus (DM), family history, chronic kidney disease (CKD), stroke (stroke), myocardial infarction (IM), blood pressure (BP).
The following data were used to assess nutritional status: waist circumference (WC-cm); hip circumference (CQ-cm); Waist/hip ratio (WHR); Waist circumference/height ratio (R CEST); taper index (CI); weight (kg) and height (m) for calculating body mass index (BMI) obtained by the formula BMI = weight (kg) / heigh²(m), where the BMI of 25 to 29.9 kg was classified as overweight / m², and as obese BMI ≥ 30 kg / m² [4]. The weight (kg) was determined using n d the digital scales (Toledo®) with the participant standing and barefoot. For height, a manual stadiometer (Alturaexata®) was used, with the individual standing, barefoot, with heels together, back straight and arms extended at the side of the body [4].
Waist circumference - WC (cm) was obtained using a non-extensible measuring tape, positioned immediately above the umbilical scar, and the reading made at the time of expiration [4,17]. The classification was carried out according to the cutoff points recommended by the World Health Organization and recommended by the Brazilian Association for the Study of Obesity and Metabolic Syndrome [4,18], to assess the metabolic risk associated with abdominal adiposity, where it was accepted the risk of metabolic complications increased for men (≥9 4 cm) and women (≥80 cm). The hip circumference (QC) was measured in the region with the largest perimeter between the waist and the thigh [4].
The waist/hip ratio (cm) for both genders was also calculated using the ratio between WC and hip circumference (QC) and classified according to the WHO cutoff points and recommended by ABESO, where the cut-off values are 0.90 cm for men and 0.85 cm for women, to observe cardiovascular risk (CVR) and metabolic syndrome, due to the accumulation of intra-abdominal fat [4,18]. Rest was found from the ratio between WC and height, both in centimeters, and values ≥ 0.52 for men and ≥ 0.53 for women were considered at risk [4].
The taper index (C index) was determined by measuring weight, height, and waist circumference, using cut-off values of ≥ 1.25 cm for men and ≥ 1.18 cm for women [19]. Obtained from the formula.
About hemodynamics, the blood pressure of the participants was checked to record the values of systolic (SBP) and diastolic (DBP) blood pressure obtained utilizing the mean of two blood pressure measurements, performed by a single evaluator, a procedure performed observing the recommendations of the VII Brazilian Guidelines on Hypertension [20].
Data analysis involved the application of descriptive statistics, and for categorical variables, relative and absolute frequencies were expressed, and for continuous variables, means and standard deviations were expressed. The diagnosis of normality was performed using the Shapiro-Wilk test, performed with the aid of the Stata ® statistical program (version 14). To investigate the possible association between the profile variables hemodinâ tamarin and other cardiovascular risk factors in overweight and normal-weight groups were used the chi-square test (x²). For the analysis of the association between anthropometric indicators and blood pressure in these two groups, the test was used, and the results were presented as mean and standard deviation. Simple linear regression was used to test the influence of anthropometric indicators on cardiovascular risk. In all tests, the level of significance was set at p-value ≤ 0.05 with a 95% confidence interval.
As for ethical aspects, the nature of the study was described for patients, and the informed consent forms were duly signed, according to CONEP Resolution 466/12. And the study has approval by the Ethics Committee in Research of the University President Dutra Hospital (CEP-HU) under number 289937 and financing by Fundação the Amparo to search (FAPEMA) - Research for SUS: shared management in of Notice FAPEMA 016/2013.
RESULTS
This study involved the participation of 171 participants, of both sexes, holders of hypertension and/or diabetes mellitus.
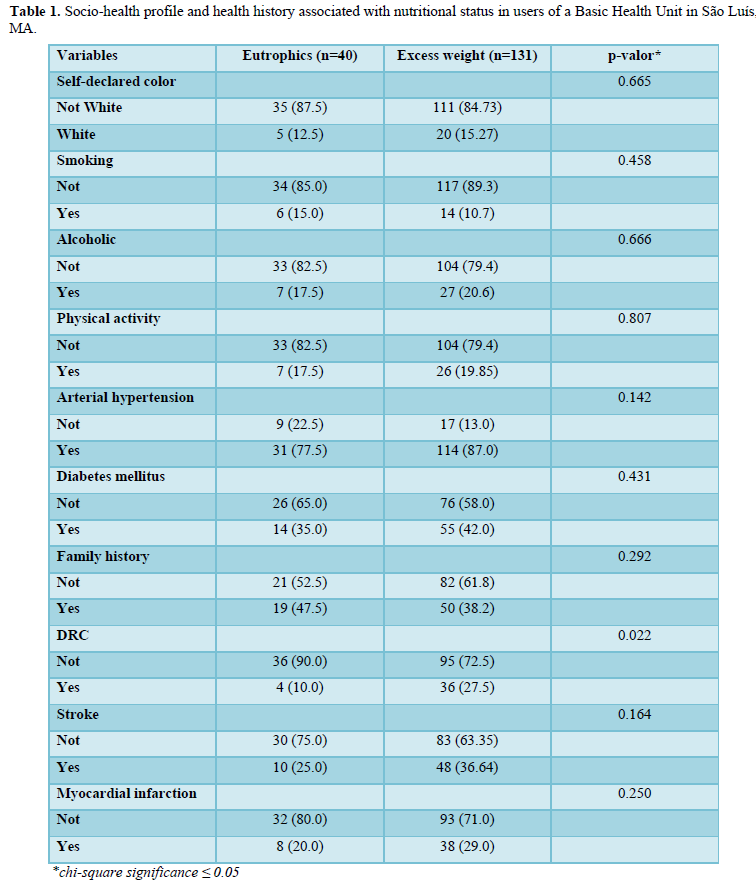
The assessment of the cardiovascular profile and risk factors demonstrated that the majority of the population studied was overweight (n = 131), female (7%), where, within this group, the majority declared themselves to be non-white (84,73%) and the assessment of lifestyle showed that participants in this group do not smoke and Will not consuming drink alcoholic 89.3% and 79.4%, respectively. As for the practice of regular physical activity in both groups (eutrophic and overweight), sedentary people prevail 82.5% and 79.4%, respectively (Table 1).
Regarding the distribution of the diseases reported by the participants (previously diagnosed), it was found that the overweight group hypertensive was more prevalent (87%) than the patients (42%). In diols are, assessment of family history made predominantly Thyroid Disease renal crony cha (CRD) with 90% and 72.5%; stroke (75% and 63.35%) and myocardial infarction (MI) 80% and 71% in the eutrophic and overweight group, respectively. With a statistically significant result only for CKD (0.02) (Table 1).
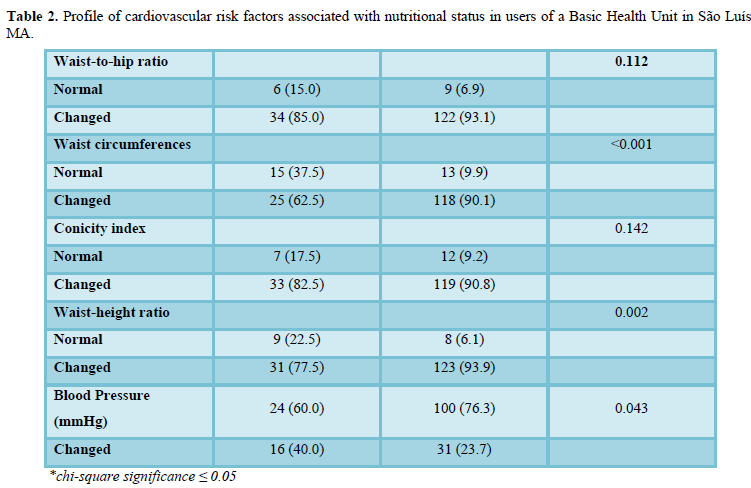
The assessment of body composition indicators showed changes in all measurements in both groups, namely, C / Q ratio, waist circumference (WC), taper index (CI), height-to-height ratio (Rest) with emphasis on the group overweight with the following respective values: 93.1%, 90.1%, 90.8%, and 93.9%, revealing that this group is more exposed to cardiovascular risk. With a statistically significant result for the variables CC (<0.001) and Rest (0.002) (Table 2). In turn, the evaluation hemodynamic demonstration that the population of two groups (eutrophic excess weight) had blood pressure changed to, especially the overweight group (76.3%), with the result statistically mean (0.043) between the groups (Table 2).
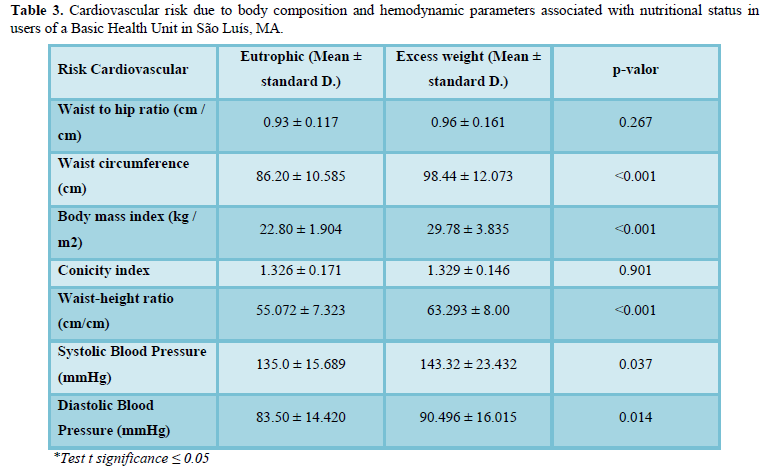
The evaluation of the cardiovascular risk by parameters of body composition and hemodynamic this study showed higher averages for the group overweight with statistical significance for the circumference’s variables waist (<0.001), relation waist-height (<0.001), speeding systolic blood (0.037) and pressure arterial diastolic (0.014). However, in the other group, despite participants and if find eutrophic most medium presented the interaction as recommended by health associations predicting exposure to cardiovascular risk (Table 3).
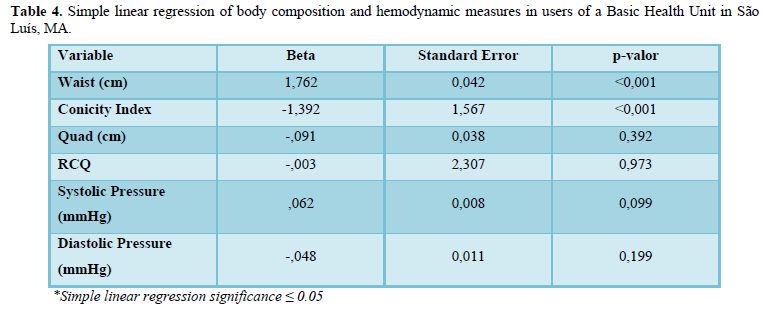
Analyzing the regression of the body and hemodynamic composition measurements, the data described the relationship statistical between the variable waist circumference (<0.001) and the conicity index (<0.001) which demonstrates higher in the degree of influence of these variables on the detection cardiovascular risk when compared to the other variables studied as shown in Table 4.
DISCUSSION
According to Abeso [4] and the Brazilian Society of Cardiology [20] exists in literature a consensus about what can justify the Rising Sunn to the overweight in incidence and prevalence in the population and the complications resulting from this state of weight at different stages of life. One of the reasons that draws attention is the routine imposed by the modern age that has reflected in society regardless of social class, amendments psychological behavior that affect the population to practice h will negative to health as food and style of inadequate life, characterized by an increase in caloric intake above the need in general from the consumption of "fast food"; disorder of hours of the main meals; energy imbalance; changes in sleep schedules and greater adherence to style sedent life are.
The placements that study since this made it possible to raise information relevant to the understanding of cardiovascular risk factors associated with nut state regional of pa participants residing in one area lacking, highlighting the high number of people with excess weight (n = 131). We observed will the implications negative health, the relationship social, labor power causes anxiety attacks, risk cardiovascular generally increased, maximizing spending on health, and reduced quality of life.
A study by Melo [21] evaluating the excess weight adults (reef), also found high levels of exception so weight 62.5% (n = 364). Silva [22] in his study on cardiovascular risk profile in patients with diabetes and hypertension in the city of Japaratinga (Alagoas), also makes approaches similar to for talecem the alarming scenario overweight growth in the country.
According to data from the National Health Survey of 2013 (PNS) indicated that 56.9% of the adult population is overweight. The results also point to a trend towards an increase in the prevalence of overweight among women over 35-44 years of age that exceeded that of men, with the highest percentage (71.4%) in the 55-64 age group [23].
According to the Abeso map [4], the northeast region had a prevalence of 44.45% overweight in adults of both sexes. Some surveys indicate that more than 50% of the population is overweight, that is, in the overweight and obesity range.
Regarding the lifestyle, the data Ever Meet augers in this study related to smoking and alcohol consumption the group's point for reduced consumption rates. These findings can be justified by the sociodemographic characteristics of the sample studied, which are mostly female in advanced age, with limited financial resources, which limits and disadvantages these habits.
And on this, Bezerra and Alencar [24] in the study of the association d the excess size and weight of the beverage servings consumed in Brazil, the s findings corroborate the consumption of large portions of liquor is positively associated with excess weight. A study by Teston [25] the study of factors associated with the disease cardiovascular references in adults found that the consumption - alcoholic beverage logic is a triggering factor for the increased weight and with a positive association with the cardiovascular risk. Studies by Sabóia [26], Ortega-Pérez [27], and Teston [25] also present similar positions regarding the contributions of alcohol in this scenario.
According to data from the Center for Disease Control and Prevention (CDC) d abandon the habit of smoking increase of approximately one-quarter of the prevalence of overweight in men and about one-sixth in women. This effect can be explained by the thermogenic effect of tobacco (nicotine), in addition to being known as appetite reducer [28]. In this context the absence of tobacco causes of abstinence crises, increases anxiety, lowers metabolism, and contributes to the increased intake the caloric and consequently the weight during adjustment phase without smoking [28]. Similarly, Christmanna [29] stud the profile of RCV of Foster in elderly lives of Guarapuava, also found low rates of retails and smoking hands and sharing opinions the like above.
As a respect, the practice of activity regular physical in both groups prevailed sedentary peoples. And Bazotte according to [30] the sedentary contributes to episodes intolerance glucose and development of diseases such as diabetes are type 2 diabetes. The diabetes is often mind correlated to physical inactivity, dyslipidemia, obesity, hypertension, which determines an increase in cardiovascular risk when compared to non-diabetic people [31]. Pinho [32] in a population-based survey (1,580 adults) found a prevalence of 51.9% (p-value <0.001) of, abdominal fat, a worrying result that justifies the efforts of researchers in the search for peaceful actions. to improve that data. Are salient, still other benefits of exercise: increase in serum HDL-C and reduction of cholesterol total (TC), LDL-c, triglycerides (TG); besides improving R function endothelial and thus act in the prevention of problems in the blood vessels, for example [4,33].
Concerning the assessment of hemodynamic where it was found that the participants in both groups (eutrophic excess weight) possessed already blood pressure, especially the group of excess weight, with a statistically significant result (0.043).
It is worth noting that the hemodynamic imbalance contributes to negative health outcomes, increases the likelihood of metabolic changes and hospital admissions, and also maximizes the need for greater financial investment in treatment (pharmacological and non-pharmacological). In addition, it maximizes the chances of heart attack and heart failure, stroke and kidney impairment.
A study by Carvalho [14] evaluating the relationship between blood pressure and indexes anthropometric the child/adolescent and behavior variables of cardiovascular risk in adulthood, shared an idea that systemic arterial hypertension has a risk-predicting behavior for other cardiovascular pathologies, which are still useful with anthropometric measures of obesity.
Silva [22] In one study in adults with hypertension and diabetes mellitus u UBS m Japaratinga-AL indicates that the lack of lev useful pressure increases the incidence of the disease and its damage to the population and the public coffers. Also making difficult treatment adherence and weight excess further contributes to this lack. On these data the Ministry of Health says that Brazil has poor control of blood pressure in the adult population (22.7%) and about 60% of older people with only a third of the disease control rates.
Concerning the measures anthropometric the results found in this study show changes in body composition indicators (C/Q; CC, IC, and WHeR) in both groups, especially the group overweight. Predicting that these patients are more exposed s to the cardiovascular risk and metabolic complications s resulting from the imbalance weight when compared to the group eutrophic, but without discarding the existing risk for the latter. The statistically significant result for DC variables (<0.001) and WHeR (0.002) in both groups show a greater association of these two measurements with Composition and greater accuracy in measuring the risk when compared to other measures, which motivates their greater use in the screening for the survey of information anthropometric data in health research.
According to Ferreira [34], Moraes [35] researches reported that the measurement of the waist circumference (WC), the ratio of the waist circumference, and hip ratio (WHR), conicity index (CI) and waist-height ratio (WHeR) is capable of identifying users at risk potential for CVD in patients with weight imbalance. This corroborates with data from studies that demonstrated that excess weight is directly related to coronary heart disease and losses for nutritional health indicators.
It is already well established that RCest is recognized as the most appreciated instrument in population-based studies and communities, as it is a simple resource, with good sensitivity and easy applicability in the field that allows to correct possible errors of WC through height and obtain more accurate results in the evaluation of abdominal obesity and the influence of risk factors for cardiovascular diseases, such as high coronary risk [26].
Regarding the altered CC rates in this study, similar results were found by Santos [36] during the evaluation anthropometry in patients overweight treated in outpatient nutrition of two hospitals in the public health of the Brazilian northeast.
According to Caetano [37], anthropometric indices have been widely used as from fat location indicators central to determine the association between excess weight and risk factors for cardiovascular diseases vascular (CVD) and then evaluate the impact on the life of individual, communities or populations to measures to prevent and or intervention can be successful.
Thus, to reestablish weight balance, several types of nutritional interventions can be used to assist overweight people and associated comorbidities. These measures use pharmacotherapeutic plans associated with dietary and sports adaptations applied according to the particularities of each individual or group that is receiving the intervention of the pharmaceutical professional, the multidisciplinary health team, or the family.
CONCLUSION
The characterization of their searched population allowed to watch a higher prevalence of overweight, non-white people, is not adept at tobacco and alcohol consumption, however, with high rates of a sedentary lifestyle in two studied groups (eutrophic and overweight).
The hemodynamics assessment of the two groups showed a higher prevalence of uncontrolled BP tension levels, especially in overweight individuals, conferring a greater risk to users' health.
It was observed that the risk of developing cardiovascular problems and metabolic complications, weight imbalance, is very much affected in this population by WC; WHR; IC and Rcest. Highlighting CC and Rcest in this study.
Therefore, it is up to the pharmaceutical professional to carry out an aligned and collaborative work with many health professionals without monitoring these patients, an end of promotion that helps to help populations adhere to healthier lifestyle habits to prevent problems with weight or even rebalancing it.
- Escobar-Cardozo GD, Correa-Bautista JE, González-Jiménez E, Schmidt-RioValle J, Ramírez-Vélez R (2016) Percentiles of body fat measured by bioelectrical impedance in children and adolescents from Bogotá (Colombia): the FUPRECOL study. Arch Argent Pediatr 114(2): 135-142.
- Sarturi JB, Neves J, Peres KG (2010) Obesity in adults: A population-based study in a small municipality in southern Brazil in 2005. Sci Collective Health 15(1): 105-113.
- Oliveira RC, Silva G, Arthur RAP, Dória H, Previato A, et al. (2013) Association between anthropometric, body composition, biochemical and food consumption measures in overweight individuals. Rev Bras Prom Saúde 26(2): 157-165.
- ABESO (2016) Brazilian Association for the Study of Obesity and Metabolic Syndrome. Brazilian obesity guidelines 2016. 4th São Paulo.
- Brazil Ministry of Health (2008) Health Care Secretariat. Food guide for the Brazilian population: promoting healthy eating. Brasília: Ministry of Health.
- Bourbon M, Miranda N, Vicente AM, Rato Q (2016) Cardiovascular diseases: do you know how to prevent it? Brasília: National Institute of Health Accessed on: December 10, 2019. Available online at: http://hdl.handle.net/10400.18/3447
- Carnelosso ML, Barbosa MA, Porto CC, Almeida e Silva S, Carvalho MM, et al. (2010) Prevalence of risk factors for cardiovascular diseases in the eastern region of Goiânia (GO). Sci Collective Health 1: 1073-1080.
- Silveira EL, Cunha LM, Pantoja MS, Lima AVM, Cunha ANA (2018) Prevalence and distribution of cardiovascular risk factors in patients with coronary artery disease in Northern Brazil. Rev da Facul Ciências Méd Sorocaba 20(3): 167-173.
- Martins AL (2018) Evaluation of the public-private relationship in cardiovascular procedures of high complexity in SUS [dissertation]. Brasília: University of Brasília.
- Tutuchima MT, Ferreira TN, Bennemann RM (2015) Association between anthropometric indicators (BMI and WC) in relation to the risk for cardiovascular diseases. Health Res 8: 55-63.
- Fraga AS, Ladeia AMT, Sa CKC, Tenorio MCC (2017) Effect of the Exercise on HDL-C Levels: A Systematic Review of Metanalysis. Rev Bras Med Esporte 23(6): 488-494. Accessed on: August 14, 2019.
- Thota P, Perez-Lopez FR, Benites-Zapata VA, Pasupuleti V, Hernandez AV (2017) Obesity-related insulin resistance in adolescents: A systematic review and meta-analysis of observational studies. Gynecol Endocrinol 33(3): 179-184.
- Lobato TAA, Torres RS, Guterres AS, Mendes WAA, Maciel AP, et al. (2014) Anthropometric indicators of obesity in patients with acute myocardial infarction. Rev Bras Cardiol 27(3): 203-212.
- Carvalho CA, Fonseca PCA, Barbosa JB, Machado SP, Santos AM, et al. (2015) Association between cardiovascular risk factors and anthropometric indicators of obesity in university students from São Luís, Maranhão, Brazil. Ciênc. saúde coletiva 20(2): 479-490.
- Pelegrini A, Silva DAS, Silva JMFL, Grigollo L, Petroski EL (2015) Anthropometric indicators of obesity in the prediction of high body fat in adolescents. Rev Paul Pediatr 33(1): 56-62. Accessed on: November 12, 2019. Available online at: http://www.scielo.br/pdf/rpp/v33n1/pt_0103-0582-rpp-33-01-00056.pdf
- Martins MA, Barbosa LB, Silva LA, Pelazza BB, Eid LP, et al. (2018) Evaluation of cardiovascular risk factors in people with diabetes mellitus and arterial hypertension in the family health strategy. Itinerarius Reflectionis 14(4): 1-20.
- Martins MV, Souza JD, Martinho KO, Franco FS, Tinôco ALA (2017) Association between triglycerides and HDL-cholesterol ratio and cardiovascular risk factors among elderly persons receiving care under the family health strategy of Viçosa, Minas Gerais. Rev Bras Geriatr Gerontol 20(2): 236-243.
- World Health Organization. Obesity: preventing and managing the global epidemic. Geneva: WHO; 1998. (Report of a WHO Consultation on obesity).
- Pitanga FJG (2011) Anthropometry in the evaluation of abdominal obesity and coronary risk. Rev Bras Cineantropom Desempenho Hum 13(3): 238-241.
- Brazilian Society of Cardiolog (2016) VI Brazilian guidelines for hypertension. Archiv Cardiol 95(1): 1-51.
- Melo SPSC, Batista Filho M, Rissin A (2015) Overweight of adults living in a subnormal urban area. Rev Bras Prom Saúde 28(2): 257-265.
- Silva DGVC (2016) Cardiovascular risk profile in patients with diabetes mellitus and arterial hypertension treated at a basic health unit in the municipality of japaratinga - AL [Course Completion Work]. Maceió: Federal University of Minas Gerais.
- Brazilian Institute of Geography and Statistics (2015) National Health Survey 2013: life cycles: Brazil and large regions [Internet]. Rio de Janeiro: Brazilian Institute of Geography and Statistics. Accessed on September 14, 2019. Available online at: https://biblioteca.ibge.gov.br/visualizacao/livros/liv94522.pdf
- Bezerra IN, Alencar ES (2018) Association between excess weight and portion sizes of drinks consumed in Brazil. Rev Saude Publica 52: 21.
- Teston EF, Cecilio HPM, Santos AL, Arruda GO, Radovanovic CAT, et al. (2016) Factors associated with cardiovascular disease in adults. Med [Internet] 49(2): 95-102. Accessed on: October 18, 2019. Available online at: http://revista.fmrp.usp.br/2016/vol49n2/AO1-Fatores-associados-as-doencas-cardiovasculares-em-adultos.pdf
- Sabóia RS, Araújo AP, Barbosa JMA, Galvão CEP, Cruvel JMS, et al. (2016) Abdominal obesity and associated factors in adults seen at a School Clinic. Rev Bras Promoç Saúde 29(2): 259-267.
- Ortega-Pérez CA, Costa-Júnior ML, Vasters GP (2011) Epidemiological profile of drug addiction in college students. Rev Latino-Am Enferm 19: 665-672.
- Dare S, Mackay DF, Pell JP (2015) Relationship between smoking and obesity: a cross-sectional study of 499,504 middle-aged adults in the UK general population. Plos One 12(2): e0172076.
- Christmanna AC, Zanelattoa C, Semchechema CC, Novello D, Shiessela DL (2013) Risk profile of cardiovascular diseases and nutritional status of active elderly people in Guarapuava. UNOPAR Cient Ciênc Biol Saúde.
- Bazotte RB (2010) Diabetic patient: pharmaceutical care. Rio de Janeiro; MedBook.
- Bertoluci MC, Rocha V (2017) Cardiovascular risk assessment in patients with diabetes. Diabetol Metab Syndr 9(1): 25.
- Pinho CPS, Diniz AS, Arruda IKG, Batista FM, Coelho PC, et al. (2013) Prevalence and factors associated with abdominal obesity in individuals aged 25 to 59 years in the State of Pernambuco, Brazil. Cad Saúde Pública 29(2): 313-324.
- Guidelines of the Brazilian Diabetes Society: 2013-2014. Sao Paulo: AC Pharmaceuticals 2014.
- Ferreira LN, Assis RC, Faria AKN, Chaves CG, Souza ASD, et al. (2017) Sociodemographic profile and clinical variables of hypertensive patients attended at the Clinica Escola de Fisioterapia of UESB. Rev Saúde 5(2): 19-25.
- Moraes KD, Araújo AP, Santos AF, Barbosa JMA, Martins MLB (2015) Correlation between body mass index and anthropometric indicators of cardiovascular risk in women. Rev Pesq Saúde 16(3): 175-181.
- Santos CM, Araújo AR, Cabral PC (2013) Anthropometric evolution of overweight patients treated at nutrition outpatient clinics. RASBRAN - Rev Associação Bras Nutr 5(1): 13-20.
- Caetano KA, Flores IA, Vilarinhos PAP, Fonseca DC, Martins ERT, et al. Anthropometric indicators and cardiovascular risk in university students: a mapping of production. Rev Cereus 10(1): 111-129.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Chemotherapy Research Journal (ISSN:2642-0236)
- BioMed Research Journal (ISSN:2578-8892)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- International Journal of Diabetes (ISSN: 2644-3031)


