Case Report
Ecthyma Gangrenosum in a Healthy 6-Month-Old Infant
3140
Views & Citations2140
Likes & Shares
Ecthyma gangrenosum (EG) is a rare, necrotizing, bacterial infection of the skin most commonly caused by pseudomonas aeruginosa. Although direct skin inoculation without septicemia is also probable, usually EG is pathognomonic for pseudomonas septicemia, which has a mortality rate at 38-96%.
Result: Herein, we report a case of previously healthy 6-month-old boy diagnosed of EG of anogenital region. Culture from the lesion revealed heavy grows of pseudomonas aeruginosa. The child responded well to antibiotic therapy.
Conclusion: It is crucial to clinically suspect EG and promptly start empiric antibiotic therapy covering pseudomonas aeruginosa to decrease the morbidity and mortality of this invasive infection.
INTRODUCTION
Ecthyma gangrenosum is a skin bacterial infection due to Pseudomonas aeruginosa. If it is a rare affection in patients with prior septicemia, it is even rarer in healthy patients. We describe the case of a healthy 6-months-old infant treated in our department.
CASE PRESENTATION
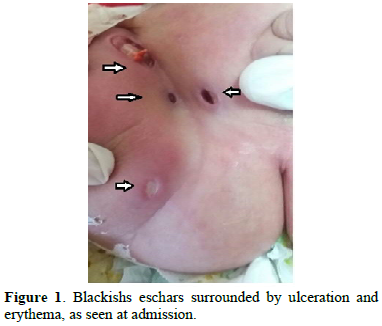
A previously healthy 6-month-old boy presented with 7-day history of fever and multiple deep, blackish eschar surrounded by extender ulceration and erythema on his anogenital region, rapidly involved despite local treatment with antiseptic (Chlorhexidine). On physical examination, weight was 9kg, body temperature 38, 5°c, pulse 120/mn, respiration rate 35 breaths/mn, and his blood pressure 80/55 mmhg. He had striking cutaneous lesions, consisting of multiple demarcated plaques with dusky violaceous erythema surrounding dry central necrotic aera in the Anogenital region (Figure 1).
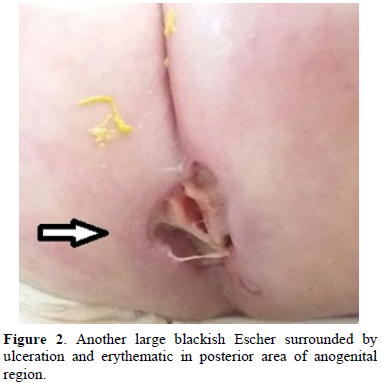
On laboratory tests, hemoglobin was 9,9g/dl, white blood cell counts, 20400/mm³ (neutrophils:45%, lymphocyte 43%), thrombocyte count, 612000/mm³, erythrocyte sedimentation rate, 30mm/1h, c-reactive protein, 7,4 mg/l. the boy was hospitalized with provisional diagnosis of EG, and empiric ceftazidime and amikacin were started. Peripheral blood cultures were negative, but a wound culture grew pseudomonas aeruginosa. The agent was susceptible to the outgoing antibiotic treatments. Antibiotic treatment was completed to 3 weeks and the boy was discharged with complete cure (Figure 2). Serum immunoglobulin’s values checked after resolution of infection turned out normal (Figure 3).

DISCUSSION
EG is a rare cutaneous infection often caused by pseudomonas aeruginosa, although other bacteria, fungi, and viruses can be responsible [1]. EG usually appears in immunocompromised patients, neutropenic being the most common risk factor in the context of either malignancy or immunosuppressive therapy [2]. It has also been reported, however, albeit very rarely, in previously healthy patients [3]. Pseudomonas aeruginosa septicemia is community-acquired in 42%, and nosocomial in 58% of patients [4]. Community- acquired pseudomonas infection can occur in healthy children, especially in young children under 1 year of age [5]. EG is a well-recognized cutaneous manifestation of pseudomonas infection with or without septicemia [6]. Clinically, EG appears as an erythematous macula with central acchymotic induration, which quickly turns into hemorrhagic bullae and then a necrotic ulcer with eschar [5,6]. It’s commonly located in the anogenital region and axillae [1, 6], but may occur anywhere else, including the face [3,7]. The lesion may be unique or multiple [3]. Early recognition and administration of appropriate antibiotic therapies is essential for EG treatment and prevention of sepsis-related death or permanent injury [1,3]. Empirical anti-microbial therapy with anti-pseudomonas penicillin and aminoglycosides should be started and adjusted on the basis of culture results [7]. Poor prognosis is associated with delay in treatment, neutropenia and mainly the presence of underlining diseases. Finally, diagnosis of EG should lower investigator’s threshold for consideration of further assessment of immune function of the affected child after acute illness [7].
CONCLUSION
This case was reported to remind that Pseudomonas aeruginosa infections may also occur in healthy children in contrast to the general opinion and to emphasize that Ecthyma gangrenosum is a finding which leads to diagnosis.
COMPETING INTEREST
The author declare that they have no Competing interests.
- Ashish P, Poonam S, Yogendra Y, Mamta D (2013) Ecthyma gangrenous in a neonate: Not always pseudomonas. BMJ Case Rep 2013: bcr2013009287.
- Akkurt ZM, Fidan V, Uçmak D, Dal T, Kelekci S, et al. (2016) A case of perineal Ecthyma gangrenosum. Turk Pediatri Ars 51: 46-48.
- Zhang Q, Smith JC, Zhu Q, Guo Z, MacDonald NE (2012) Five-year review of pseudomonas aeruginosa bacteremia in children hospitalized at a single center in southern China. Int J Infec Dis 16: e6 28-32.
- Wu CT, Huang JL (2010) Multiple Ecthyma gangrenosum in a healthy infant with community-acquired pseudomonas aeruginosa sepsis. Pediatr Emerg Care 26: 750-751.
- Gargouri L, Maaloul I, Kamoun T, Maalej B, Safi F, et al. (2015) Ecthyma gangrenosum: A manifestation of community-acquired Pseudomonas aeruginosa septicemia in three infants. Arch Pediatr 22(6): 616-620.
- Biddeci G, Cutrone M, Mattei I, Valerio E, Favot F (2015) Ecthyma gangrenosum of the cheek in a 6-month-old infant. Arch Dis Child 100(1): 55-56.
- Grisaru-Soen G, Lerner-Geva L, Keller N, Berger H, Passwell JH, et al. (2000) Pseudomonas aeruginosa bacteremia in children: Analysis of trends in prevalence, antibiotic resistance and prognostic factors. Pediatr Infect Dis J19(10): 959-963.



QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Clinical Trials and Research (ISSN:2637-7373)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)
- Journal of Spine Diseases


