2864
Views & Citations1864
Likes & Shares
Some of them are congenital as amelogenesis imperfecta and Molar-Incisor Hypomineralization, others are acquired as tooth wear, tooth decay and tooth fracture [1,2].
Dental trauma may cause a wide degree of damage to anterior teeth, ranging from a mild concussion to varying amounts of lost tooth structure through fracture to the crown and/or root [3].
In addition to that, dental trauma may yield tooth discoloration with different varieties: white, yellow, brown, pink, gray, or black. Localized discolored teeth can be managed by minimally invasive treatment options such as resin infiltration, microabrasion, macroabrasion or bleaching and restorative methods when there is tissue loss such as composite, veneers, and full coverage crown [4].
Direct restoration with composite requires practitioner's skills to achieve an esthetic and functional morphology. However, composite is prone to discoloration which affects color stability. Thus, ceramic veneers offer the best solution in terms of esthetic results and represent the least invasive restorative approach. Moreover, in some cases, other alternatives as full coverage crowns should be envisaged to restore fractured teeth and protect the residual dental structure [1,4,5].
Various factors need to be considered while developing a treatment plan for fractured and discolored teeth [6].
CASE PRESENTATION
A 24-year-old female patient attended to the department of fixed prosthodontics for restoring her fractured central incisor because of its unaesthetic appearance (Figure 1). Thermal and electric pulp testing revealed that the tooth was necrotic.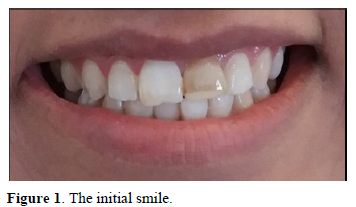
The patient’s anamnesis revealed that the tooth had been fractured 2 years ago during an accident. Direct composite restorations had been placed one month after the trauma. The patient had no complaint, except for the unaesthetic appearance due to the dyschromia of the fractured incisor. A zirconia-based crown was indicated (Figure 2).
Before tooth preparation, root canal treatment was done. The defective composite was removed and the tooth was prepared (Figure 3).
Thereafter, a glass fiber post was placed. The esthetic core was built up with composite resin and bonded with self-adhesive bonding resin (Figure 4).

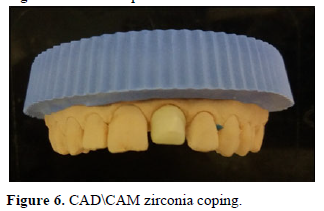
After master impression (Figures 5 & 6), working cast was performed, and scanned. A zirconia-based crown was milled by CAD/CAM.
Then, the crown was checked intraorally and the entire cementation procedure was performed. A three-month follow-up asserted complete patient satisfaction with regard to her smile (Figure 7).

DISCUSSION
Traumatic injuries to anterior teeth are frequently encountered in our daily practice. The tissue damage depends on the direction and severity of impact. It can be a simple fracture with loss of enamel, and it can also be a most serious injury which can reach the pulp [1].
A comprehensive clinical examination involving vitality test findings, dislocation of teeth, percussion analysis findings, and injuries of periodontal tissues, is crucial to determine the appropriate treatment plan [2].
There are many treatment options available for tooth fractures. They are mainly:
- Tooth fragment rebonding
- Composite resin restorations
- Veneers
- Full-coverage crowns
The selection of the right therapeutic option depends on the fracture line’s position (Table 1).
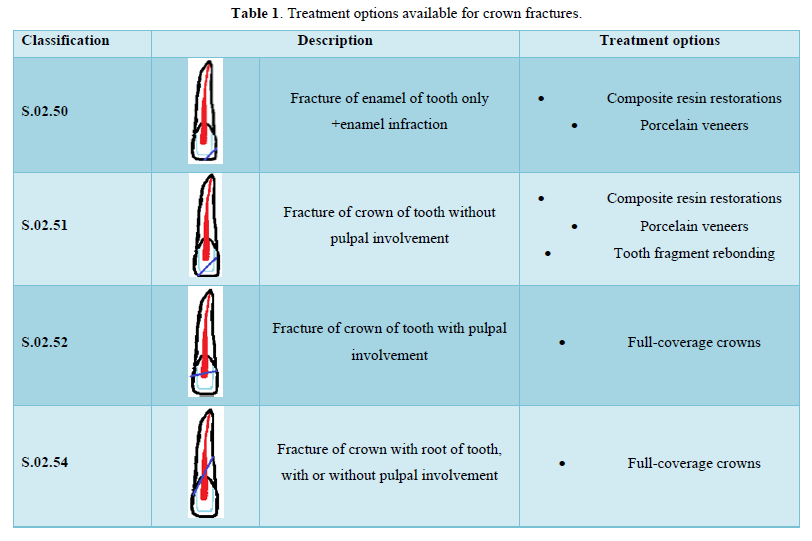
Tooth fragment rebonding is the most conservative restorative option. However, many studies showed that rebonding of fractured fragments has a mean value of resistance to fracture that is lower than both intact teeth and teeth restored with ceramic veneers [5].
The study of Stellini [3] showed that the resistance of teeth with rebonded restorations is 54.9% of that of, intact teeth, which was lower than the resistance of teeth restored with ceramic veneers (81.8% of that of intact teeth).
Ceramic veneers showed higher resistance than fragment rebonding and esthetic qualities with a long-term outcome.
According to the study of Meijering AC et al. the survival rates were 94% for porcelain restorations, 90% for indirect composite restorations and 74% for direct composite restorations.
While ceramic veneers are the most conservative, economical and safe treatment options for the management of fractured teeth, in some cases, other alternatives as full coverage crowns should be envisaged to restore fractured teeth and protect the residual dental structure [1].
Crown discoloration is a common sequel following trauma, teeth may become yellow, gray, brown, black, or pink [7,8].
The alteration in color may be caused by Enamel hypoplasia, Internal/external resorption, calcific metamorphosis, Dentin hyper-calcification and Intra-pulpal hemorrhage where hemoglobin and erythrocytes are released. The penetration of hemosiderin into the dentine can lead to a change in crown color [9].
This sequel evolves in more than 90% progressing to non-vitality and pulp necrosis. Also, since exposed pulp and/or non-vital teeth are sources of chronic infection and discomfort, affected teeth should be treated [10].
Treatment of localized tooth discoloration is challenging and requires a well knowledge of material properties used for treating the tooth defect. The ability of the material to mask the discolored substrate and, at the same time, match the color of adjacent teeth is crucial to the treatment's success.
In our clinical case, the discoloration of the fractured teeth required a combination of endodontic treatment and restoration with 3Y-TZP zirconia based crown.
The study of Basegio [10] evaluating the masking ability of different prosthetic material on tooth colored resin substrates showed that samples of veneered 3Y-TZP zirconia had a better masking effect than monolithic lithium disilicate, translucent zirconia, hybrid ceramic, or heat-pressed ceramic over Translucent zirconia samples [11,12].
Additionally, inner zirconia with veneering glass ceramic could provide a suitable esthetic outcome.
CONCLUSION
The restoration of discolored and fractured teeth may require minimally invasive or more extensive treatment modalities with a multidisciplinary approach. The success of these treatments relies on good choice of the prosthetic material that can mimic mechanical proprieties and esthetic qualities of an intact tooth and mask the discoloration.
Informed Consent Statement: Not applicable.
Data Availability Statement: The data presented in this study are available on request from the corresponding author.
Conflicts of Interest: The authors declare no conflict of interest.
- Chafaie A (2016) Esthetic management of anterior dental anomalies: A clinical case. Int Orthod 14(3): 357-365.
- Yildirim Z, Gomec OY (2017) Treatment approaches for traumatized anterior teeth with excessive tissue loss: Three case reports. J Istanb Univ Fac Dent 51(2): 54-60.
- Stellini E, De Francesco M, Sivolella S, Ferro R, Denotti G, et al. (2012) Experimental evaluation of two methodologies for the restoration of crown fracture in permanent anterior teeth. Eur J Paediatr Dent 13(2): 91-96.
- Wang C, Jia X-T, Zhen M, Hu W-J, Zhang H, et al. (2022) Success rate of fractured teeth receiving modified crown lengthening surgery and restorations. BMC Oral Health 22(1): 99.
- Surekha GL, Vinay C, Baliga S, Uloopi KS, RojaRamya KS, et al. (2021) Effect of preconditioning the fractured coronal fragments with remineralizing agents on fracture resistance of re-attached teeth. J Indian Soc Pedod Prev Dent 39(4): 384-387.
- Dey S, Saluja I, Thomas M (2021) Localized dental dyschromia-causes and management. Gulhane Med J 63: 238-245.
- Holan G (2004) Development of clinical and radiographic signs associated with dark discolored primary incisors following traumatic injuries: A prospective controlled study. Dent Traumatol 20: 276-287.
- Aldrigui JM, Cardioli IC, Mendes FM, Antunes JL, Wanderley MT (2013) Predictive factors for pulp necrosis in traumatized primary incisors: A longitudinal study. Int J Paediatr Dent 23: 460-469
- Moccelini BS, de Alencar NA, Bolan M, Magno MB, Maia LC, et al. (2018) Pulp necrosis and crown discoloration: A systematic review and meta-analysis. Int J Paediatr Dent 28(5): 432-442.
- Basegio MM, Pecho OE, Ghinea R, Perez MM, Bona DA (2019) Masking ability of indirect restorative systems on tooth-colored resin substrates. Dent Mater 35: e122-e130.
- Gasparik C, Manziuc MM, Burde AV, Ruiz-López J, Buduru S, et al. (2022) Masking Ability of Monolithic and Layered Zirconia Crowns on Discolored Substrates. Materials (Basel) 15(6): 2233.
- Manziuc MM, Gasparik C, Burde AV, Ruiz-López J, Buduru S, et al. (2022) Influence of manufacturing technique on the color of zirconia restorations: Monolithic versus layered crowns; J Esthet Restor Dent 34(6): 978-987.
-
 Table 1
Table 1








QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Clinical Trials and Research (ISSN:2637-7373)
- International Journal of AIDS (ISSN: 2644-3023)


