Case Report
Comparative Study of Conventional and Modified Arch Bar with Screw in Maxillomandibular Fixation
1257
Views & Citations257
Likes & Shares
Objective: IMF/maxillomandibular fixation (MMF) is considered one of the most important steps in the management of maxillofacial trauma. The objective of this study is to compare time of placement and removal, wire prick injury and oral hygiene in patients having conventional arch bar and modified arch bar with screw in maxillomandibular fixation.
Material and methods: Twenty two patients who reported to our Department with mandibular fractures and required intermaxillary fixation were selected and randomly divided into 2 groups of 11 patients each that is Group A and Group B. Group A included patients who received intermaxillary fixation with modified arch bar with screws and Group B who received intermaxillary fixation with conventional arch bar. The parameters compared in both the groups included, time of placement and removal of arch bar, gingival index and wire prick injury.
Results: The average surgical time taken and wire prick were more in Group B, the patient acceptance and oral hygiene was better in Group A.
Conclusion: Intermaxillary fixation with modified arch bar with screws is more efficacious compared to conventional arch bar in the treatment of mandibular fractures.
Keywords: Wire prick, Oral hygiene, Modified arch bar, Gingival index, Intermaxillary fixation
Abbreviation: IMF: Intermaxillary Fixation; MMF: Maxillomandibular Fixation; Pre-Op; Pre-Operative; Post-Op: Post-Operative
INTRODUCTION
Evolution has made humans quite susceptible to frontal impacts. Trauma to the facial region is common in road traffic accidents, sports‑related injuries, and assaults. Maxillofacial trauma represents 42% of all injuries. In these, 70% are mandibular fractures and 30% are maxillary fractures. Since the ancient times, intermaxillary fixation (IMF) has been used alone to treat fractures of maxilla and mandible. Treatment of maxillofacial fractures depends on reduction and fixation using open or closed techniques and on restoration of normal occlusion. Before fracture reduction, temporary intermaxillary fixation (IMF) with correct registration of occlusion is necessary [1].
Various methods to achieve IMF have been described in literature such as Ivy eyelet wiring, Risdon wiring, arch bars, metal splints, acrylic splints, gunning type splints for edentulous patients, bonded brackets, and more recently self‑tapping and self‑drilling MMF screws. Erich arch bars have been considered as the standard for achieving MMF because of its rigidity and versatility [2]. Although they provide superior occlusion control and reliable fixation, they have many disadvantages including difficulty in maintaining oral hygiene, trauma to the periodontium, reduced patient compliance and discomfort, longer time required for placement, and risk of needle stick injury.
The aim of this article is to compare conventional arch bar with modified arch bar in intermaxillary fixation in terms of time taken for placement and removal, oral hygiene and wire prick injury.
MATERIAL AND METHODS
Twenty two patients who reported to our Department with mandibular fractures and required intermaxillary fixation as a part of treatment plan followed by open reduction and internal fixation under GA were selected and randomly divided into 2 groups of 11 patients each that is Group A and Group B. Group A included patients who received intermaxillary fixation with modified arch bar with screw. Group B includes patients who received intermaxillary fixation with conventional arch bar. The parameters compared in both the groups included, time of placement and removal of arch bar, gingival index preoperatively and post operatively and wire prick injury.
Surgical technique in fixation of conventional arch bar
- Procedure was done under all aseptic precautions.
- All the patients were treated using 2% lignocaine hydrochloride with adrenaline in 1:200000 concentrations (Lignox 2% -A) or intraoperatively during open reduction and internal fixation of the fractures under GA.
- Arch bar was taken according to the desired length.
- 15cm 26 gauge pre stretched 18-8 stainless steel wire was taken.
- Wiring of the tooth was done from 1st molar to 1st molar in both arches. Arch bar was placed in position, upper bar hook should be facing up and lower bars hook should be facing down and secured in position by wiring it to the neck of the teeth.
- Wiring was done in such a way that, the wire was passed from the mesial surface of the tooth to lingual side and back on the buccal side from distal surface of the tooth, one end of wire was above the bar and one end was below.
- Securing of the bar was done by twisting the wire in clockwise direction so bar is attached securely and firmly to the neck of teeth on buccal surface.
- IMF was attained by securing the hooks with tie wires on either side.
Surgical technique in fixation of modified arch bar
- Procedure will be done under all aseptic precautions (Figure 1).
- All the patients were treated using 2% lignocaine hydrochloride with adrenaline in 1:200000 concentrations (Lignox 2% -A) or intraoperatively during open reduction and internal fixation of the fractures under GA.
- Careful evaluation of inter-radicular space for drilling.
- Modified arch bar was taken according to the desired length and adapted to match the contour.
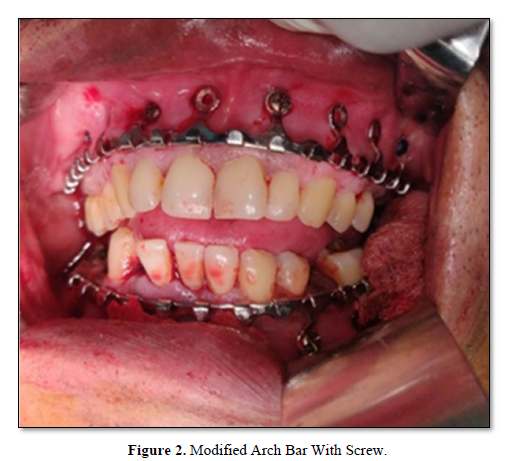
- Modified arch bar was placed in position and fixed by 1.5x8 mm screws in three areas where the perforation had been made, and if necessary, more screws can be placed taking care that all the screws are placed in the inter radicular spaces (Figure 2).
- Arch bar was held in such a way that upper bars hook was facing upwards and lower bars hook was facing downwards.
- Screws were not over tightened in order to prevent ischemic necrosis.
- If the first hole is centered between the incisors, a sufficient number of holes will be coincident to inter-radicular spaces required for fixation of the arch bar.
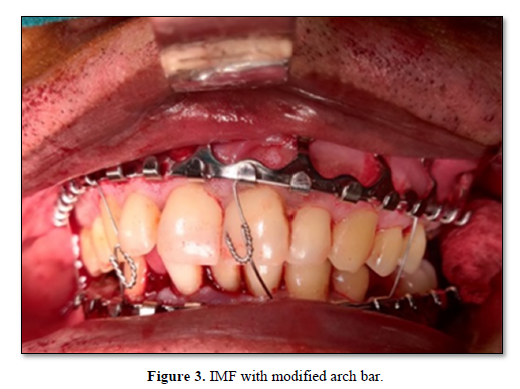
- IMF was attained by securing the hooks with tie wires on either side (Figure 3).

RESULTS
Descriptive statistics was performed for the parameters assessed in different groups. Intergroup comparison for different parameters was assessed using unpaired t-test/independent samples t-test. All statistical tests were performed at 95% confidence intervals; keeping p value of less than 0.05 as statistically significant.
In Group A, mean age of patients was 32.53 years in comparison to 33.40 years in Group B, indicating no significant difference in the age of two groups (P = 0.8827). In Group A, of 11 patients treated, 7 (63.6%) were males and 4 (36%) were females; in Group B, 8 (72%) patients were male and 3 (27%) were females (P = 0.771) which shows statistically insignificant.
The criteria measured between two groups are described below:
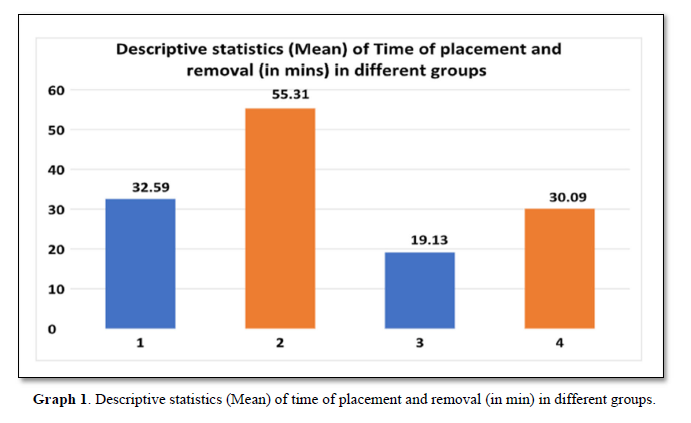
1. Time of placement and removal of arch bar
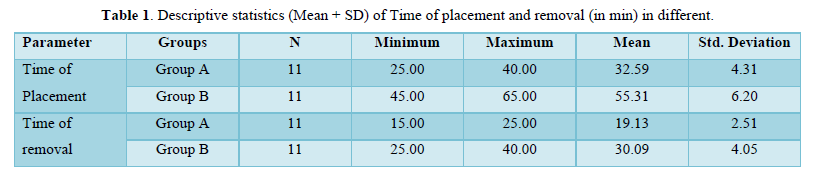
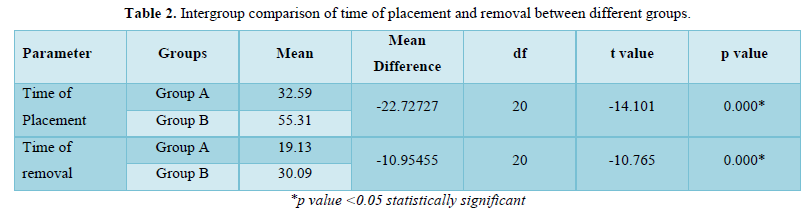
The average time of placement of arch bar in Group A (modified arch bar) is 32.59±4.31min while the average time of placement of arch bar in Group B(conventional arch bar)is 55±6.21min which is 1.6 times of group A. Similarly, average time of removal of arch bar in Group A is 19.13±2.51 min, while average time of removal of arch bar in Group B is 30.09±4.05min which is 1.6 times of group A. *p value (Tables 1,2 & Graph 1).
 2. Gingival index
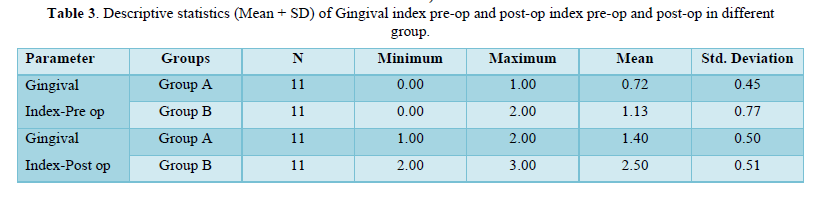
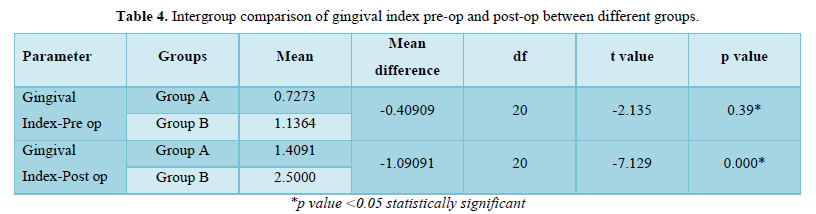
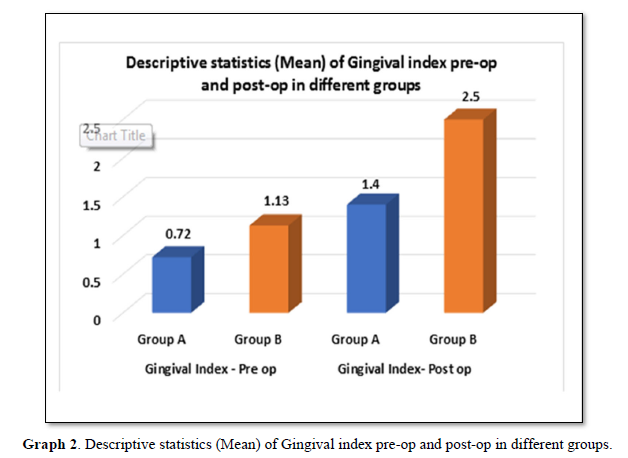
2. Gingival indexThe average gingival index preoperatively in Group A is 0.72±0.45 and post operatively it is 1.40±0.50 while in Group B average gingival index preoperatively is 1.13±0.77 and post operatively it is 2.50±.51 which indicates that the patients having modified arch bar have comparatively better oral hygiene than patients having conventional arch bar.*p value (Tables 3,4 & Graph 2).
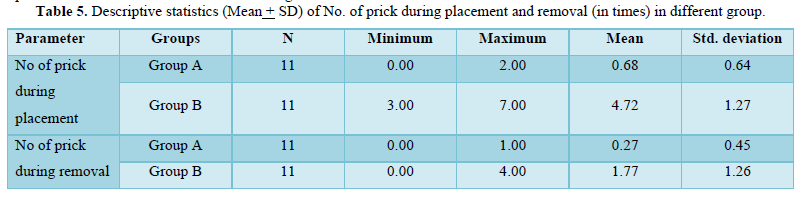
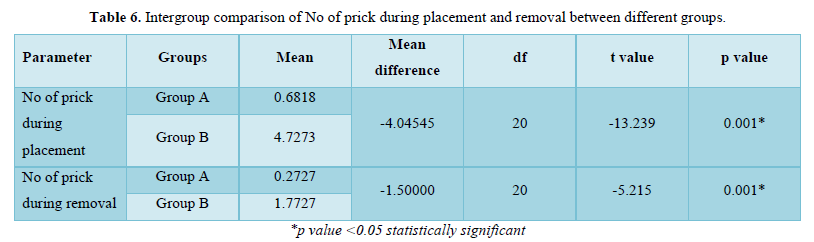
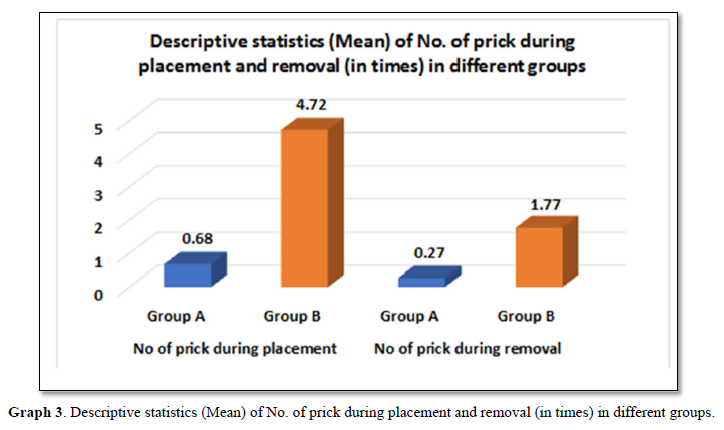
3. Number of pricks during placement and removal
The average number of prick in group A during placement of arch bar is 0.68±0.64times and removal is 0.27±0.45times, while in group B number of pricks during placement is 4.72±1.27 times and during removal it is 1.77±1.26 times which is 7 times more than Group A. *p value (Tables 5,6 & Graph 3).
DISCUSSION
Treatment of mandibular fractures has been in a constant state of evolution over the last few decades [3]. The main aim of treating mandibular fractures includes fracture site reduction, stabilization, and achievement of correct dental occlusion. During this process, it is also advantageous to use methods that decrease the risk of percutaneous transmission of blood–borne diseases, operating time and maintenance of oral hygiene. The management of maxillofacial fractures includes different techniques from closed reduction to open reduction and internal fixation and requires control of the dental occlusion with the help of IMF which is time‑consuming with the use of conventional techniques [4].
Moreover, conventional arch bar technique is difficult to use when the teeth are grossly carious, periodontally compromised, crowded and have extensive crown and bridge work in the oral cavity [5]. Final tightening of wires during the placement of conventional arch bars around the teeth may cause “necrosis of the mucosa,” “extrusion,” and subsequent loss of vitality of the tooth. It is also not easy to maintain the gingival health [6].Wires have to pass below the gingival margin to guarantee stability, chances of gingival injury are more and compromises the health of periodontium, rounded wire edges collects food debris and causes gingival inflammation and difficulty in maintaining oral hygiene result in fetid breath [7].
To overcome the drawbacks of conventional arch bars, the modified arch bar was introduced in the year 2016 by Qureshi [8] Similar modified arch bar was used by Anna [9] and named it as SMART lock hybrid arch bar [9]. Bone anchored arch bars combine 2 methods for reducing mandibular fractures: conventional arch bars and MMF screws. The advent of MMF screws has circumvented many challenges inherent to the use of arch bars. MMF screws have significantly reduced the risk of penetrating injury to the surgeon, surgical time, and trauma to the gingiva [8].
In this study, the time taken for the placement of conventional arch bars and modified arch bar with screw was noted. The data showed that average time 55.31±6.20 was required for the placement of conventional arch bar(Group B) while the average time for the placement of modified arch bar (Group A) was found to be 32.59±4.31 min, which suggested reduced intraoperative time and shorter duration of general anesthesia by 1.6 times. Similarly in conventional arch bar(GroupB) removal the average time was 30.09±4.05 min while in modified arch bar removal(Group A) average time taken was 19.13±2.51min which interprets statistically significant differences(p value<.05) between the two groups for time of placement and removal.
In the present study, the most common complication that occurred with the use of modified arch bar with screws was screw loosening. At the 14th postoperative day, screw loosening was seen in 2 (18%) out of 11 patients. Out of the total number of screws placed (70) in our study, 7 (10%) screws became loose at the end of 2nd week. Screw loosening mainly occurs due to the force exerted by the oral musculature, while the patient is in IMF.
It can also occur when the direction of screw is not perpendicular to the occlusal plane [9].
Another complication that occurred with the use MMF screws was the coverage of the screw head with oral mucosa. Rai [6] reported a high incidence of mucosal coverage of the screws. In our study, Out of the 70 screws used in the study, 22 (31%) screws were completely submerged in oral mucosa at the end of 4th week. According to Rai [6] the cause behind the high occurrence of this complication was perhaps the IMF screws were placed high up in the movable alveolar mucosa rather than in the adherent mucosa [9].
In this study oral hygiene was also compared in both groups modified versus conventional arch bar using gingival index grading 0,1,2 and 3. It was seen that average gingival index of patient having modified arch bar (Group A) was 0.72±0.45 before arch bar placement and1.4±0.50 after conventional arch bar placement which is twice of previous while average gingival index of patients having conventional arch bar (Group B) was1.13±0.77 before arch bar placement and 2.5±0.51 after arch bar placement so the mean difference between two group preoperatively is -0.409 and postoperatively-1.09 which interprets-statistically significant differences (p value<0.05) between the groups for gingival index preoperatively and postoperatively.
In the present study wire prick injury was also a parameter for comparison between conventional and modified arch bar during placement as well as removal of arch bar. It was seen that average number of prick in modified arch bar (Group A) during placement was 0.68±.64 while in conventional arch bar (Group B) it was 4.72±1.27 which is 7 times of modified arch bar while average number of prick in Group A during removal was 0.27±0.45 and in Group B it was 1.77±1.26 so the mean difference between two groups during placement was-4.045 and mean difference during removal of arch bar was -1.5 which interprets statistically significant differences(p value<.05) between two groups for number of pricks during placement and removal the maximum wire prick in patient with conventional arch bar was 7times during placement and 4times during removal while in modified arch bar during placement 2 times and during removal hardly any prick (3 out of 11) injury occurred.
The results achieved with the present study indicate that modified arch bar with screw technique is a good alternative to conventional arch bars for temporary IMF in mandibular fractures. It is a safe and time sparing technique, oral hygiene is well maintained and incidence of prick injury to the operator is also low compared to conventional arch bar however, it is not without limitations or potential consequences which the surgeon must be aware of to provide safe and effective treatment.
CONCLUSION
Modified arch bar with screws provide an effective alternative to conventional arch bar technique for IMF in the treatment of uncomplicated mandibular fractures. However, modified arch bar with screws are not indicated where the function of tension band and postoperative directional traction are required as in multiple comminuted mandibular fractures, pediatric patients with unerupted teeth, and patients with severe osteoporosis. Although modified arch bar with screws offers many advantages over the conventional arch bar, large sample size studies are required to prove its efficacy.
ACKNOWLEDGEMENT
All authors have viewed and agreed to the submission.
CONFLICT OF INTEREST
There is no conflict of interest.
- Agarwal M, Meena B, Gupta DK, Tiwari AD, Jakhar SK (2014) A prospective randomized clinical trial sscomparing 3D and standard miniplates in treatment of mandibular symphysis and parasymphysis fractures. J Maxillofac Oral Surg 13: 79‑
- Jones DC (1999) The intermaxillary screw: A dedicated bicortical bone screw for temporary intermaxillary fixation. Br J Oral Maxillofac Surg 37(2): 115-116.
- Nandini GD, Balakrishna R, Rao J (2011) Self tapping screws v/s Erich arch bar for inter maxillary fixation: A comparative clinical study in the treatment of mandibular fractures. J Maxillofac Oral Surg 10: 127-131.
- Gibbons AJ, Baden JM, Monaghan AM, Dhariwal DK, Hodder SC (2003) A drill‑free bone screw for intermaxillary fixation in military casualties. J R Army Med Corps 149: 30‑3
- Tracy K, Gutta R (2014) Are embrasure wires better than arch bars for intermaxillary fixation? J Oral Maxillofac Surg 15: 45‑
- Chandan S, Ramanojam S (2010) Comparative evaluation of the resin bonded arch bar versus conventional Erich arch bar for intermaxillary fixation. J Maxillofac Oral Surg 9: 231-235.
- Qureshi AA, Reddy UK, Warad NM, Badal S, Jamadar AA, et al. (2016) Intermaxillary fixation screws versus Erich arch bars in mandibular fractures: A comparative study and review of literature. Ann Maxillofac Surg 6: 25-30.
- Carlson AR, Shammas RL, Allori AC, Powers DB (2017) A Technique for Reduction of Edentulous Fractures Using Dentures and SMARTLock Hybrid Fixation System. Plast Reconstr Surg Glob Open 5(9): e1473.
- Rai A, Datarkar A, Borle RM (2011) Are maxillomandibular fixation screws a better option than Erich arch bars in achieving maxillomandibular fixation? A randomized clinical study. J Oral Maxillofac Surg 69: 3015‑3018.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6












QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)



